Interview with Joe Kvedar, MD, President, American Telemedicine Association (ATA) Professor of Dermatology, Harvard Medical School Physician Scientist, Author. As the only organization completely focused on advancing telehealth, the ATA is committed to ensuring that everyone has access to safe, affordable, and appropriate care when and where they need it, enabling the system to do more good for more people.
Honora Miller:
Dr. Kvedar, thank you for joining us.
Dr. Kvedar:
I’m delighted to be with you.
Honora Miller:
Can you tell us what telemedicine is?
Dr. Kvedar:
Well, it’s not a new concept, but since the late 1960s, people have been talking and working towards this idea that care doesn’t necessarily have to be two people in the same room at the same time — that we can use technology to connect people. Like we’re doing now with this video interview, that’s the most common type of telehealth visit, but we can also connect with patients via telephone calls.
There are various remote monitoring devices that are able to monitor an individual’s vital signs or other health measures in their homes.
Finally, in the same way we exchange emails and text messages, we can do that securely with patients, what we call e-visits, which can be very helpful, as well. So there are a variety of forms, but it’s really all about care where the patient is, when the patient needs it, and not having an individual travel to visit a doctor in person.
Honora Miller:
Can you break down the differences between the terms telehealth, virtual visits, e-visits, and virtual health?
Dr. Kvedar:
I’ll go back to the beginning when there were visionary clinicians who believed medicine could be delivered this way and were doing this kind of work. They called it telemedicine. A few years into that journey, there were a number of clinicians who felt that the same technologies could be used in other ways, including education, and so they started using the term telehealth to make it broader and more inclusive. To this day, telehealth the term that everyone is mostly comfortable with.
A few years ago, some people started to say that we needed to be able distinguish between real-time and asynchronous interactions, the same way that we have video or phone calls and emails, and that we also needed to distinguish between direct-to-patient interactions and interactions between clinicians
If it is an interaction between patient and doctor, it’s a virtual visit; if it’s between clinicians, it’s a virtual consult. For example, if a physician is caring for a stroke patient in another hospital, we call that a virtual consult. An e-visit is considered an asynchronous interaction. For instance, I’m a dermatologist, so if my patient takes a picture of a rash or skin disorder, and sends it to me via a secure portal, I could respond with a message back to the patient. That would be an e-visit.
Likewise, if the primary care doctor caring for a patient decided that she wanted a picture of something looked at and sent it to me electronically, then we call that an e-consult.
Telehealth generally encompasses four areas: virtual visits, virtual consults, e-visits and e-consults. Digital Health has become a term of art because that includes everything from robotic process automation, to artificial intelligence, and so on.
Honora Miller:
What is telemedicine remote monitoring?
Dr. Kvedar:
Well, remote monitoring is best suited for certain conditions, mostly chronic illness — conditions like congestive heart failure or high blood pressure or diabetes, particularly type 2 diabetes, when it’s helpful to have more data from the patient about their condition.
For example, if you were starting out on blood pressure medication, we could give you a blood pressure cuff to take home, so that you could take your blood pressure for a week. The cuff, connected by Bluetooth, would automatically share your BP readings with your healthcare provider.
That would be an example of home-monitoring. For people with heart failure, we might give them a wireless blood pressure cuff, weight scale and a device to measure oxygen levels in the blood, so that we can remotely monitor their vital signs.
There are a variety of opportunities to monitor all types of health measures using wearable devices like an Apple Watch, and sensors, that can remotely monitor things like an EKG, sleep patterns, daily activity and other functions.
Honora Miller:
Is the monitoring done in real-time? Or do patients supply the data as it becomes available by entering it into a portal?
Dr. Kvedar:
A lot of remote monitor is done in an asynchronous way. For example, you might step on a scale every morning, take your blood pressure and heart rate, and that personal health data is securely transmitted to your healthcare provider and winds up in your electronic health record. Then a nurse or other provider could look at your data and put in a call to you if something was not quite right, and you’d have a dialogue. Again, it could be a video call or an audio call, but you’d have a dialogue with your provider about what was going on — maybe your diet was off, or maybe you need to increase your medicine dose, but that’s typically how it’s done. It’s not usually done with real-time readings.
Honora Miller:
Can you speak to what telemedicine care looks like in the era of COVID-19?
Dr. Kvedar:
I’ll start with statistics from my own large delivery system in Boston to give you a flavor, and by the way, our numbers are not unique. February of 2020, across two academic hospitals, we did about 1600 virtual encounters. In March, we did 89,000 and in April we did 242,000. We are not unique because I’ve been talking to my colleagues around the country and everyone’s having that kind of accelerated demand for telehealth services, what we would call hockey stick growth, partly because, to help stop the spread of the virus, people need to stay at home, yet we still have to take care of our patients. The technology that you and I are using for this interview is common now, whether it be Zoom or Skype or FaceTime.
People are, for the most part, comfortable with video calls, and likewise, patients have really taken to it. Patients generally have been very, very positive. Doctors are warming to it. Many doctors are saying Gosh, there’s so many things I can do this way that I hadn’t thought about, and I’m going to continue to practice this way. So telehealth services have grown a like wildfire. Before the pandemic, mental health was the biggest user and for sure now mental health providers are still the biggest users of telehealth. In mental health care, providers are talking to the patient, so it’s very easy to make that transition. And then we mentioned chronic illness before, but it turns out that the screening questions used to decide if someone needs a COVID test can easily be asked via telehealth.
if someone is sick at home with only mild symptoms, that individual can be monitored quite well using this kind of virtual care tool set because it’s all about asking questions.
Honora Miller:
So those are the main things that we’re seeing — the use of telehealth for follow-up visits for all kinds of conditions and health concerns, mental health, as well as respiratory symptom questions to determine if individuals need additional testing for coronavirus.
I’m wondering if you can speak to whether or not health insurance coverage has kept up with the pace of change in this arena?
Dr. Kvedar:
So great question and any time you ask about insurance coverage, it is always a long answer with a lot of caveats. I’ll start with Medicare, the Centers for Medicare and Medicaid Services, the biggest payer in the country for the elderly and disabled, and they said very early on they would pay for telehealth at the same level they would pay us for seeing you in the office, so that was a big boom. They’ve since refined that to pay for telephone calls at that rate, as well. That, by the way, is really a nod to addressing disparities because there are people who can’t afford a smartphone or have broadband and we want to make sure that we get to them.
I credit the Medicare folks for seeing that. Medicare is doing very well. Medicaid is state-by-state. Reimbursement will depend upon where you live. But most states, most governors, during this State of Emergency, said that they should pay and most private payers are paying for telehealth as well, so it’s pretty rosy right now, in terms of reimbursement.
One of the things that we’re doing at the ATA is trying to make sure that enough of that reimbursement culture sticks when we move out of this health crisis so that people can continue to enjoy the benefits of this type of care delivery.
Honora Miller:
Do you think that there will be legislation required in order to have that level of coverage continue or is there going to be another mechanism to advocate for that to be the case?
Dr. Kvedar:
Again, great question. I would say that if we look at history as a guide, when Medicare decides to pay for something, private payers typically follow, and there was no need for legislation because it was something that just rippled through the medical economy. So that’s what we’re hoping will happen again. In every state Medicaid is a little bit different. Patients have found that they can get care and there’s this what I call the magic of access, quality and convenience. And when you get that kind of care delivery, everyone feels great about it.
Patients have experienced that and doctors have experienced that. I would just suggest that you listeners and readers talk to their company’s human resources person, and tell them how much they’ve enjoyed their telehealth benefit; if you are insured by the government, take the time to write your senator or representative, and tell them that you don’t want to go back to in-person only care. I think we will have to advocate some but there’s such an overwhelming positive response that I’m quite optimistic that it will stick.
Honora Miller:
Having recently experienced four or five different medical professionals interacting with me through telemedicine, I’ve noticed that there’s a different cadence to each of the visits depending on the person’s communication style and their comfort level with the medium.
How patients can prepare themselves in order to get the best possible experience out of telemedicine?
Dr. Kvedar:
Sure, but before I get to that, I would just quickly say that we’re working on doctors, too, on what we’re calling “website manner.” It used to be something that we sort of said with a chuckle, but we’re very serious about it now. And it’s things like looking directly at the camera, and dressing up so that your patient takes you seriously.
But back to your question about how patients can prepare for a telehealth visit. I’d suggest everyone think about being more conscious of the information that your doctor needs to help you, either in making a diagnosis or by helping you with a care plan. For example, when we were able to have office visits back in the day — that was only several weeks ago — the doctor was asking questions, they listened to your lungs, your heart, even indicators such as your speech pattern or if you look your doctor in the eye. They were collecting information constantly during that office visit. So, let’s say, you’re a patient with diabetes. You should make sure you have your blood sugar readings handy.
Let’s say you’ve been following your blood pressure, make sure you have your blood pressure readings handy.
For me, as a dermatologist, it’s so important that we have good images of whatever it is on your skin that you need looked at. So it’s really thinking through what information your provider needs, and sometimes a doctor will help you. In our case, in advance of a telehealth interaction, we send patients information about how to take good quality pictures of their skin condition. So we’re learning, too.
Also, make sure you have your questions ready in advance, which is always good advice, both for an in-person or virtual visit, so that you get all your questions answered.
Make sure you have all the information about your condition that you can gather and make sure you have your questions prepared.
Honora Miller:
In relation to lab tests that a patient may need to get, how does that work in the telemedicine context?
Dr. Kvedar:
Well, that’s a wonderful question. Notwithstanding home pregnancy tests and the like, there are a number of companies making great strides towards taking a drop or two of blood and having a test done in the home, so we can look forward to that in the future.
In the meantime, the answer is, you need to go to a lab, hospital or clinic for testing, which is in most cases what happens currently. Things like genetic tests can be done with saliva, so some samples can be packaged from the home and shipped to a lab to be evaluated.
So it depends on the test, but unfortunately, for a lot of these tests, we still have to send people to a lab to get a blood specimen drawn or to leave a urine or stool specimen.
Honora Miller:
How can patients best identify whether their doctors provide a telemedicine option?
Dr. Kvedar:
Well, these days, I think most doctors are being very proactive, because we have this dilemma, where we want to take care of you but we’re discouraging you from coming to healthcare facilities because of the risk of contracting the virus.
If your doctor hasn’t reached out to you and you feel like you need a consultation or some care, reach out to your doctor and ask them what telehealth platform they’re using.
The government also said in the middle of March, when they relaxed the reimbursement rules, that providers could use any technology right now that we wanted during this crisis, including FaceTime, Skype, Google Hangouts, Zoom et cetera.
I’ve been telling patients, if you’re comfortable, there’s no harm in asking your doctor’s office if they will talk with you via FaceTime or another platform. I would say the first step is to ask your provider. Most people can also get access to basic telehealth services through large pharmacy chains. If you happen to have a CVS app on your phone or a Walgreens app, you can get a telehealth visit that way as well.
Most health plans, even before this health crisis, would offer an option for you to get a telehealth visit. I hope your doctor is responsive and he/she should be, but in the event that your provider isn’t offering telehealth visits, other options exist.
Honora Miller:
Can you speak to what tools a patient will need to adequately engage with patient portals?
Dr. Kvedar:
Patient portals have been around for a long time. However, I would give us a bit of a black eye on making them user-friendly. I don’t think we’ve done a very good job of that. And again, this is a patient empowerment conversation, and I don’t know that we’ve done a very good job of empowering people to interact with us through those tools.
That said, all of a sudden now patient portals have become a primary way you’re interacting with your healthcare providers, so we’re upping our game. It’s too bad it takes a crisis but there it is, and I think we’ll get much, much better.
I often say, every service you consume other than healthcare has a digital front end that has a way of interacting with software to get things done easily. For example, you take a picture of your check and deposit in your bank account with just a few taps on your smartphone. There’s millions of examples now, and health care is just getting going in that regard.
The patient portal story is really mostly about security, that is to say, it’s a very secure electronic environment for you to interact with your healthcare provider. The basic things that you can do there, apart from doing a virtual visit, is to do billing information, usually there’s a way to get a list of your medications, ask for prescription refills, schedule appointments, get letters for things like school physicals, and that the like. Nowadays, those things can be handled electronically.
There’s a little bit of, I would say, activation energy for some people, because signing up can be complicated.
It is so secure you are sometimes required to submit a letter or do something extra than you would to sign up for a normal website, all in good intent. I would urge people to put up with whatever barrier hits you in the beginning. Once you get involved with a patient portal, and we’re working very hard now to make it a really a good experience for you, patients will be able to not only interact with us as providers, but you will be able to access all kinds of information and services offered by your healthcare system, access lots of information from your record and so forth.
Honora Miller:
As a cancer patient, and for others living with chronic conditions, how might telemedicine impact the future of survivorship?
Dr. Kvedar:
It’s a great question. One aspect of survivorship is things like living wills which, if it isn’t done electronically, we will have to move in that direction, to enable that. There is a lot of interest in interactivity with palliative care and hospice around how to better care for patients, particularly around medication management. Patients can be afraid of opiates and sometimes they’re in terrible pain, so we need to get this right. So those are a couple of examples.
Honora Miller:
Is a potential for telemedicine to be used in lieu of in-person visits to such an extent that the medical provider doesn’t get to see the patient enough to pick up on subtleties that are crucial? Can you share any insights about this concern?
Dr. Kvedar:
I think that’s wonderful insight and we are definitely grappling with that for sure, especially now that telehealth use has surged. Before this pandemic hit, we had only one channel healthcare delivery to come to the hospital or doctor’s office. Now of course the answer is, let’s do a telehealth visit.
But the truth is somewhere in the middle, and I trust clinicians to have good instincts about that.
For instance, patients that we’re treating for a chronic illness, maybe we do every other visit in the office so that we can have that face time and actual interactivity. There’s something about in-person interactions with patients that’s very special. I take care of patients with acne, for example, and arguably that can be done online. But I would say we’ll probably end up doing every other visit in the office, because you want to get to know the patient, their family, etcetera. It’s just that right now where we don’t really have a choice.
Honora Miller:
Can you speak to privacy concerns around telemedicine?
Dr. Kvedar:
Forty-eight states have temporarily loosened their licensure restrictions in response to the pandemic. As, a patient, that may or may not hit your radar, depending upon where you live. Here in Eastern Massachusetts, I have a medical license in Massachusetts, but regularly take care of patients who live in New Hampshire and Rhode Island, because they often had come in for office visits. So now if we’re doing follow-up care, there’s a mechanism where I can still take care of them, even though I don’t have a medical license in those two other states.
Waiving restrictions on state licensure is important to point out because it’s really enabling us to again deliver better care to more people. The question then becomes, after this crisis is over, will we have to go back to the very old-fashioned, state-by-state geographic border-based care delivery model? This is something that the ATA is working on, as well as the need to maintain patient privacy, especially for providers using telehealth for the first time, who may not be familiar with these new procedures.
I would also point out that the biggest part of health data security is how we record that visit in the medical record, and that hasn’t changed. We do that in a very secure way. It’s something we take very seriously. And I don’t mean to say that you’d never get hacked. It’s part of reality that anyone can get hacked any time, but I don’t believe it’s something that should get in the way of delivering care.
Honora Miller:
Thank you, these are interesting times and we are moving at an amazing speed, and just the incredible growth that you described it really is a testament to how there can be interesting unintended consequences of a pandemic. Thank you very much for joining us and for you sharing your expertise.
Dr. Kvedar:
It’s been a real honor and pleasure.









 “It feels so good,” I said during our telemedicine appointment, “to be away from the hospital for eight weeks in a row.” It’s the longest hospital break I’ve had since being diagnosed with cancer last summer. Before mid-March, I’d been to four to ten medical appointments every month. Being a cancer patient felt like a full or half time job. Because of the pandemic, I’m now treated by my oncology team from the comfort of my own home.
“It feels so good,” I said during our telemedicine appointment, “to be away from the hospital for eight weeks in a row.” It’s the longest hospital break I’ve had since being diagnosed with cancer last summer. Before mid-March, I’d been to four to ten medical appointments every month. Being a cancer patient felt like a full or half time job. Because of the pandemic, I’m now treated by my oncology team from the comfort of my own home. My partner drove me to the hospital on the morning of my surgery. We checked in before 6a.m. and waited, with others, in the lobby.
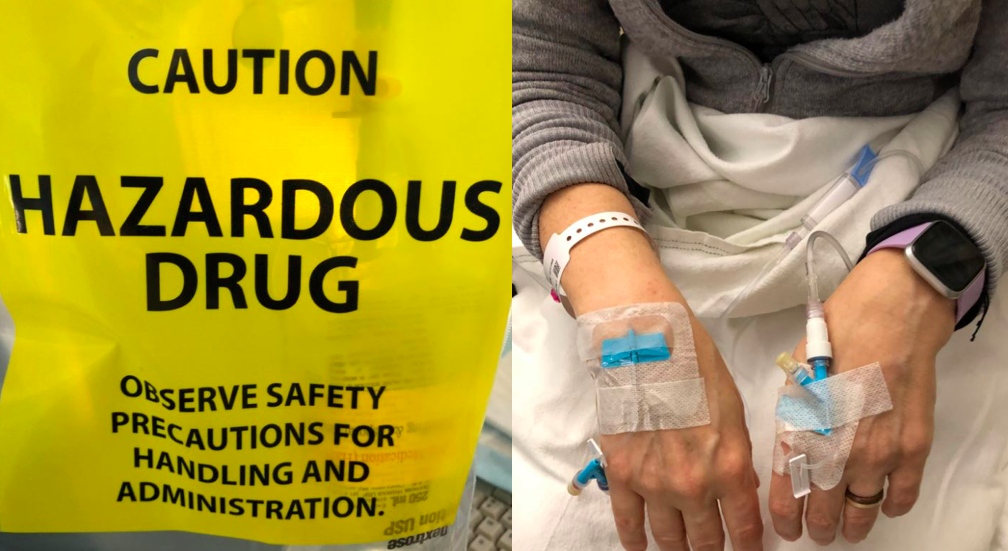
My partner drove me to the hospital on the morning of my surgery. We checked in before 6a.m. and waited, with others, in the lobby. This is me in post-op. My partner took this photo on his phone and was able to share it with my family and friends to let them know I made it through surgery. They were worried because it went hours longer than expected.
This is me in post-op. My partner took this photo on his phone and was able to share it with my family and friends to let them know I made it through surgery. They were worried because it went hours longer than expected. Going home after surgery is comforting and scary. My right leg was giving out from under me because my obturator nerve “got heat” during my surgery. I had trouble standing in the shower or lifting my right leg onto the bed or into a car. I had extensive swelling and bruising on my right side and pelvic area and had a bit of a reaction to the bandage tape. I didn’t know what was normal. And after a phone call to the hospital, I was asked to come back in for a check-up.
Going home after surgery is comforting and scary. My right leg was giving out from under me because my obturator nerve “got heat” during my surgery. I had trouble standing in the shower or lifting my right leg onto the bed or into a car. I had extensive swelling and bruising on my right side and pelvic area and had a bit of a reaction to the bandage tape. I didn’t know what was normal. And after a phone call to the hospital, I was asked to come back in for a check-up.