What Myeloma Patients Need to Know About Bispecific Antibodies from Patient Empowerment Network on Vimeo.
What should myeloma patients know about bispecific antibody therapy? Expert Dr. Jeffrey Matous explains the function of bispecific antibodies, reviews the risks and benefits of this treatment option, and provides questions to ask your doctor to help guide your care.
Dr. Jeffrey Matous is a myeloma specialist at the Colorado Blood Cancer Institute and the assistant chair in myeloma research for Sarah Cannon Research Institute. Learn more about Dr. Matous.
See More from Evolve Myeloma
Related Resources:
Transcript:
Katherine:
Let’s switch gears now to another therapy we’ve been hearing about: bispecific antibodies. One has been recently approved for myeloma, teclistamab (Tecvayli), so let’s start with what are bispecific antibodies and who might they be right for?
Dr. Jeffrey Matous:
And strap on your seatbelt, because there’s a whole bunch of them coming, I think, for approval. So, the T-cell redirecting antibodies, it’s a different strategy for trying to get your T cells, the patient’s T cells, to attack the myeloma cells. And in CAR T-cell therapy, it’s a single infusion. That’s the treatment. And the bispecific antibodies that I often call T-cell redirecting antibodies, because they redirect the T cells to the myeloma cell, these are given over a continuous period and it might as long as you tolerate it, as long as it’s working. It might be for a year. And they are given either under the skin as a subcutaneous injection, or in the vein.
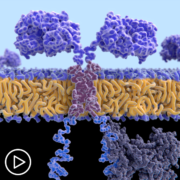
And there are many, many different of these T-cell redirecting antibodies, the bispecific antibodies. How they work, I just do this with my patients. I hold up my hand and I say the bispecific antibodies have two hooks on them, and one hook recognizes the T cell and latches onto the T cell, and the other hook latches onto the myeloma cell. And then, what it does, it brings the T cell in proximity to the myeloma cell. Then, the T cell says “Oh, aha. I’m supposed to kill this myeloma cell,” and usually does it. Now, the part that connects the T cell and these bispecific antibodies is always the same. It’s CD3. However, the part that sticks on the myeloma cell, there are different targets, and you referred to teclistamab, which was approved by the FDA, and that attaches to something on the outside of a myeloma cell called BCMA, BCMA.
But we know that other bispecific antibodies that can attach to different markers or antigens on the outside of the myeloma cell and affect the same change, and so, I think these are going to be coming fast and furious.
Katherine:
Who’s this class of treatment right for?
Dr. Jeffrey Matous:
I think – well, again, the FDA approval right now is for people who have seen pretty much everything. You know, you’ve had a lot of treatments. You’ve seen all the different classes of the myeloma drugs, but in our clinical research trials right now, we’re testing these as an initial therapy, in second-line therapy, after stem cell transplants. They’re being tested pretty much in every scenario right now in clinical trials, so right now, it’s when you’ve exhausted the normal treatments and you’re considering CAR T-cell therapy, or you’re considering getting treated with a drug called selinexor (Xpovio), or looking at another clinical trial. That’s when it’s the time to ask about the bispecific antibodies.
Katherine:
What are the risks and benefits of this therapy?
Dr. Jeffrey Matous:
The risks are pretty similar to the risks from CAR T-cell therapy, so Cytokine Release Syndrome. That usually occurs during the first week. Neurologic toxicity is, I think, less frequent with the bispecific antibodies, but infections and low blood counts definitely a concern with these bispecific antibodies, requires a lot of monitoring without any doubt.
Now, the other thing about the bispecific antibodies, there’s, right now, they’ve been in the realm of the larger centers, so myeloma centers is where people have been getting these bispecific antibodies, but there’s absolutely no question in my mind that these bispecific antibodies are going to be available through almost every general hematology, oncology practitioner’s office, but not for a while. The docs that aren’t used to giving these medicines are a little – they’re being quite cautious rolling them out in their practices right now. There are still a lot of questions as these roll out, and so, right now, I think teclistamab is still largely unavailable outside myeloma centers, but that’s going to change, I think, even over 2023 and definitely into 2024.
Katherine:
Okay. That’s really good news. For patients who want to know more about bispecifics, what questions should they be asking their healthcare team?
Dr. Jeffrey Matous:
Again, the same thing is – the same questions. Well, teclistamab is approved by the FDA. What other bispecifics are there? What about combinations? What about clinical trials? And then, that’s what you want to ask for sure. Then, how often do I need to come in the office? With teclistamab, the answer is weekly.
If they say for how long, it’s until it quits working or you have side effects, and then you can’t take it anymore. That’s the way the FDA label is. And so, it’s a big commitment to go on these treatments, but they’re effective. You ask me about the effectiveness of these drugs and, essentially, all the studies with these different bispecifics, including teclistamab, have been studied initially in people who have seen every myeloma treatment. They’ve had an average of about six different myeloma treatments.
They’ve seen all the drugs. They’re not working anymore. They’re in trouble. They’re in a pinch, and roughly, seven out of ten people have dramatic responses to these bispecifics when they’re treated, which we’ve never had anything like this at all in the myeloma world.
Katherine:
Wow. Do the side effects go away at some point?
Dr. Jeffrey Matous:
The side effects are completely manageable. Yeah and you can – by and large, you can adjust the bispecific, either the schedule or different things, to make these completely tolerable for patients.
Katherine:
Okay.
Dr. Jeffrey Matous:
Very few patients on our trials, with these bispecifics, who we have not been able to manage and, pretty much, handle all the – any side effect that occurs.