Thyroid Awareness: January and Beyond
This post was originally published by Sharon O’Day on MedicareGuide on January 21, 2021 here.
Most people with thyroid disease don’t even know they have it. More than one in eight Americans will develop a thyroid condition during their lifetime, but up to 60% are unaware of it.1
That’s because the symptoms — fatigue, depression, sleep disturbances and weight loss or gain, among others — could just as well be signs of other medical conditions and life stages.
That’s what makes Thyroid Awareness Month, which falls in January each year, so important. If both people and doctors think of thyroid problems more often, cases can be diagnosed earlier and the disease can be managed sooner.
What Is Thyroid Disease?
Thyroid disease is a medical condition that keeps your thyroid from producing the right amount of the hormones needed by your body’s systems to function. This small, butterfly-shaped gland at the lower front of your neck affects how well every cell, tissue and organ in your body works.

Photo by Torten Dettlaff
The cause of thyroid disease is unknown, but it can often be managed with medical attention. But first it has to be diagnosed through blood tests, imaging (scans or ultrasounds) and physical exams.
With hypothyroidism, the gland doesn’t make enough thyroid hormone and you can feel tired, gain weight and feel the cold more intensely.
On the flip side, when the gland produces too much hormone you can develop hyperthyroidism, leaving you feeling tired and nervous. You may also lose weight and find your heartbeat is rapid.
Graves’ disease is a specific form of hyperthyroidism, an autoimmune genetic disorder that affects about 1% of the U.S. population.2
Women are five to eight times more likely than men to be among the estimated 20 million Americans with a thyroid condition.3
Different types of benign (non-cancerous) growths and malignant (cancerous) tumors can develop in the thyroid gland. Thyroid nodules, for example, are common and usually benign; these lumps can be solid or filled with fluid. You should still seek immediate medical attention because, while most growths don’t turn out to be cancer, some do.4
What About Thyroid Cancer?
When the cells in the thyroid grow out of control, the disease can become thyroid cancer. In 2017, the latest year for Centers for Disease Control statistics, more than 33,000 women and nearly 12,000 men were diagnosed with thyroid cancer.5
Thyroid cancer has more specific symptoms than other forms of thyroid disease: a lump or swelling on the side of the neck, trouble or pain breathing or swallowing and a hoarse voice.6
What Are the Trends in Thyroid Cancer?
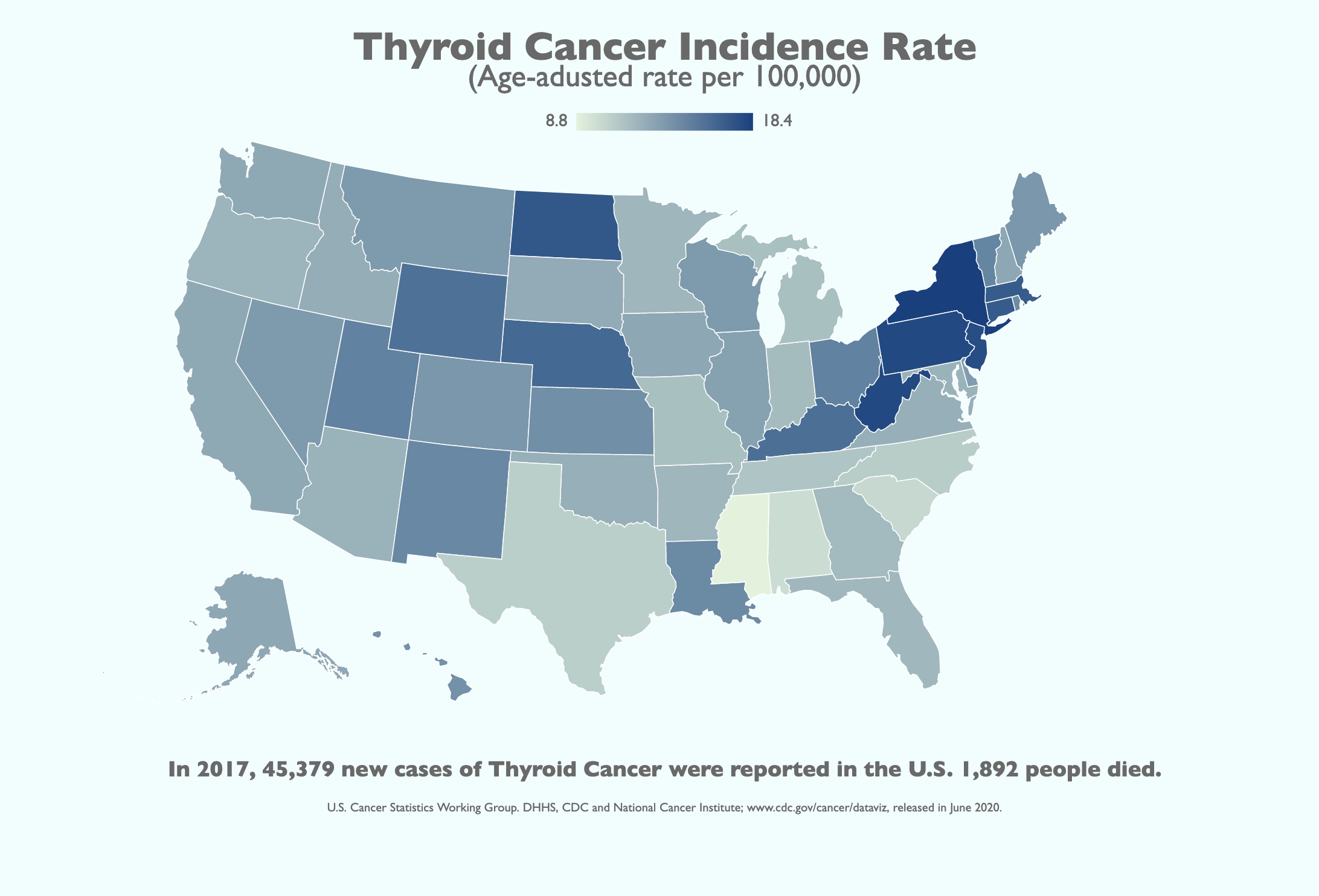
The yearly number of new thyroid cancer cases in the U.S. has grown steadily, from 18,000 in 1999 to a peak of 49,500 in 2015, with a small drop-off after that.7
In 2017, for every 100,000 Americans, 14 new thyroid cancer cases were reported and one person died.8
Scientists aren’t sure what causes thyroid cancer. But the risk factors include:9
- Being female.
- Being between the ages of 25 and 65.
- Being exposed to radiation as a child.
- Having a history of an enlarged thyroid.
- Having a family history of thyroid disease.
- Having certain genetic conditions, including familial medullary thyroid cancer (FMTC), multiple endocrine neoplasia type 2A syndrome (MEN2A) and multiple endocrine neoplasia type 2B syndrome (MEN2B).
Gender and Race
The chances of a thyroid cancer diagnosis are nearly three times higher for women than for men.10
But if you’re Black or American Indian/Alaska Native, you have about a 45% lower chance of being diagnosed with thyroid cancer than if you’re white, Asian/Pacific Islander or Hispanic.11
Survival Studies
Three factors influence the five-year survival rate for thyroid cancer patients: gender, age and race.12
- Survival rates are higher for women than for men: 98% versus 93.6%.
- Survival drops as people age, from 99.4% for those under 45 to 86.1% for those over 75.
- Survival is slightly lower for Blacks compared with whites and people of other races/ethnicities.
For women, thyroid cancer has the highest five-year survival rate of all cancers. For men, only prostate cancer and testicular cancer have higher survival rates.
Regional Glances
Across all ages, genders, races and ethnicities, the rate of new cancers is higher in the extended New England area and some western and midwest states, including Utah, Wyoming, North Dakota and Kansas.13
How You Can Raise Awareness About Thyroid Disease
Thyroid Awareness Month highlights the crucial role the thyroid plays in the ability of major organs to function. It aims for more people to get tested if they have unexplained symptoms like those mentioned above. And it promotes early treatment.
As with any type of cancer, greater awareness leads to earlier detection, which can save lives. A cancer stage is defined by whether cancer cells have been contained within the thyroid or traveled to other parts of the body, which influences your treatment options as well as the odds of recovery.14
If you want to participate in Thyroid Awareness Month, here are six simple ways to get involved:
- Do a thyroid neck check. You’ll need a hand-held mirror and a glass of water. Tip your head back, take a sip of water and swallow. Using the mirror as you swallow, watch the lower front of your neck for any bulges or protrusions. If you see any, talk to your physician right away.
- Encourage friends and family to get tested. Although symptoms are pretty general, if a loved one complains of feeling cold, not sleeping well or having trouble swallowing, ask them to do the at-home neck check and suggest they see their doctor.
- If you can, donate. Even if thyroid disease hasn’t affected you directly, consider donating to:
-
- The American Thyroid Association (ATA): The ATA’s purpose is to improve the lives of those living with thyroid disease and cancer through research, awareness and education. Visit this link for donations.
- Thyroid Cancer Survivors’ Association (ThyCa): ThyCa provides education and comfort to all people diagnosed with thyroid cancer and their loved ones. Visit this link for donations.
- Thyroid, Head & Neck Cancer (THANC) Foundation: Apart from being a major fundraiser for thyroid, head and neck cancer research—like finding new treatments and better therapies—THANC focuses on community awareness and education, as well as patient outreach and support initiatives.
- Share information online and off. ThyCa offers free materials to increase awareness of thyroid issues. Order some today and help spread the word.
- Share Your Thyroid Story. Paloma Health developed a video campaign that invites people to share their thyroid story to help raise awareness for thyroid disease symptoms, risk factors and treatment options. According to the organization, when someone submits a story, they’re automatically entered for a chance to win a thyroid support bundle giveaway.
- Use hashtags to raise awareness on social media. By using these designated hashtags from the ATA and ThyCA, your efforts to raise awareness will be multiplied:
- #thyroid #hypothyroidism #thyroidhealing #thyroidproblems #thyroiddisease #thyroidhealth #autoimmunedisease #hormones #hyperthyroidism #hypothyroidism #hashimotos #cancer #thyroidcancer #autoimmune #thyroidweightloss #covid #hashimotosdisease #thyroidwarrior #thyroidawareness #thyroidectomy #hypothyroid
Next Steps
January is Thyroid Awareness Month and September is Thyroid Cancer Awareness Month. But your efforts to raise awareness are needed year-round because most thyroid disease cases go undetected in their early stages.
Check yourself regularly with the swallow test. It only takes a minute or two. And stay vigilant when friends and family mention unexplained symptoms. If the signs fall in general categories such as fatigue, depression, sleep disturbances and weight loss or gain, encourage them to visit their doctor to have their thyroid checked.
Your efforts to promote Thyroid Awareness Month can help reduce the number of Americans who have a thyroid problem but don’t know and don’t get checked before a very treatable issue becomes much more serious.
- American Thyroid Association. “General Information/Press Room.” thyroid.org (accessed December 18, 2020).
- “General Information/Press Room.”
- “General Information/Press Room.”
- American Cancer Society. “What Is Thyroid Cancer?” cancer.org (accessed December 18, 2020).
- Centers for Disease Control and Prevention. “United States Cancer Statistics: Data Visualizations.” gis.cdc.gov (accessed December 18, 2020).
- Centers for Disease Control and Prevention. “Thyroid Cancer.” cdc.gov (accessed December 18, 2020).
- “United States Cancer Statistics: Data Visualizations.”
- “United States Cancer Statistics: Data Visualizations.”
- National Cancer Institute. “Thyroid Cancer Treatment (Adult) (PDQ®)–Patient Version.” cancer.gov (accessed December 18, 2020).
- “United States Cancer Statistics: Data Visualizations.”
- “United States Cancer Statistics: Data Visualizations.”
- “United States Cancer Statistics: Data Visualizations.”
- “United States Cancer Statistics: Data Visualizations.”
- “Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974-2013.”
Do You Need to See an Endocrinologist for Your Thyroid Disease?
This resources was originally published by the Verywell Health here.
In most cases, the diagnosis of a thyroid condition is made by a person’s primary care doctor, who may then refer you to an endocrinologist, a physician who treats hormone problems like thyroid disease and others. But that’s not always the case—or necessary. Sometimes, your general practitioner is comfortable managing your thyroid condition on his own, and this is perfectly sensible for certain thyroid diagnoses.
There are other healthcare practitioners, such as naturopaths and chiropractors, who also treat thyroid patients. While their expertise may be helpful as a complement to your thyroid care, it should not be a substitute for that of a primary care doctor or endocrinologist.
How to Work With Your Thyroid Medical Team
As managing thyroid disease can be challenging and is, in most cases, a lifelong commitment, it’s important to have the right team of professionals helping you along the way.
Thyroid Disease Doctor Discussion Guide
Get our printable guide for your next doctor’s appointment to help you ask the right questions.
:max_bytes(150000):strip_icc():format(webp)/illo_Doctor-discussion-guide-01-5c3e5b20c9e77c00015d2ba5.png)
Primary Care Doctors
Your primary care doctor may be able to manage your thyroid disease, especially if you are diagnosed with hypothyroidism. This is because most primary care doctors are comfortable and trained to monitor thyroid stimulating hormone (TSH) levels and adjust thyroid hormone replacement medication accordingly
That said, there are some specific situations that warrant a referral to an endocrinologist.
- If you are pregnant or planning pregnancy
- A newborn or child with a thyroid condition
- Presence of thyroid nodules or an enlarged thyroid gland (goiter)
- Any type of hyperthyroidism, including Graves’ disease
- Secondary hypothyroidism (if a pituitary problem is causing hypothyroidism)
- Thyroid eye disease
- Suspected thyroid cancer
Endocrinologists
An endocrinologist is a doctor who completes training in internal medicine (like a primary care physician) and then undergoes more training (usually two to three years) in the field of endocrinology.
Endocrinologists diagnose and treat hormonal imbalances, usually due to various gland conditions, such as:
- Thyroid disorders
- Diabetes
- Osteoporosis and bone health
- Adrenal disorders
- Pituitary disorders
- Menopause issues in women
- Testosterone problems in men2
While primary care doctors can manage some endocrine conditions, like “textbook” hypothyroidism and diabetes, other conditions warrant the care of an endocrinologist, like pituitary or adrenal gland problems or hyperthyroidism.
Even if you have “textbook” hypothyroidism, do not be surprised if your primary care doctor refers you to an endocrinologist. This can be for a number of reasons—perhaps you have multiple other medical problems (making your case a complex one), or perhaps your doctor does not have a lot of experience treating patients with such a disorder.
Sometimes, primary care doctors simply want an “extra set of eyes” from an endocrinologist, whether that’s taking a second look at your diagnostic test results and/or modifying your treatment plan—all of this is OK, if not, a sign of good care.
Depending on your diagnosis and treatment plan, your endocrinologist may opt to manage your condition on his own, as in the case of Graves’ disease or monitoring thyroid nodules.
Alternatively, your endocrinologist may work alongside your primary care doctor to manage your condition. For example, your primary care doctor may refer you to an endocrinologist for an initial diagnosis of Hashimoto’s disease. Once your endocrinologist stabilizes your thyroid hormone replacement dose, your primary care doctor may then follow your TSH levels. You may then only see your endocrinologist if a problem arises, or once a year for a check-in.
Other Practitioners
Many thyroid patients look to seek out 360-treatment plan—that is, one that includes the expertise of practitioners of different disciplines and takes a “whole body” approach. Naturopaths and chiropractors are two professionals who are sometimes consulted.
If you consult with these or other practitioners, be sure that you only do so as an adjunct to your care by a primary care doctor or endocrinologist. He or she should also be aware of any treatments recommended by other clinicians.
Naturopathic Doctors
A licensed naturopathic doctor (ND) graduates from a four-year graduate level holistic medical school. Their approach to healthcare tends to be more integrative perhaps than traditional doctors in that NDs believe no part of your body operates in complete isolation from the rest of the system.3
So, for example, an ND may discuss the aspects of how nutrition affects thyroid disorders and make sure that you have a diet plan that works to support your thyroid health. In addition, by ordering labs and imaging tests, an ND may evaluate other hormones such as the sex hormone estrogen and cortisol (the “stress hormone” produced by your adrenals glands).
Complement to Your Thyroid Care
While an integrative approach to your thyroid health is appealing, NDs do not necessarily follow the guidelines recommended by professional societies like the American Thyroid Association (ATA) or the American Association of Clinical Endocrinologists (AACE).
For instance, for the treatment of hypothyroidism, many NDs prescribe desiccated thyroid hormone, which is derived from the dried thyroid glands of pigs or cows and provides both T4 (thyroxine) and triiodothyronine (T3). Alternative names include natural thyroid, thyroid extract, porcine thyroid, pig thyroid; brand names include Nature-throid and Armour Thyroid.
This type of thyroid hormone replacement medication provides a ratio of T4:T3 that is not natural to humans (4:1 instead of 16:1), which tends to produce some degree of hyperthyroidism. That is why most expert bodies (the AACE and ATA, for instance) do not recommend its usage, except for perhaps select patients. Instead, for the vast majority of patients, experts recommend sticking with levothyroxine alone (brand names: Synthroid, Levoxyl, and Tirosint).4
Lastly, some NDs practice botanical medicine, recommending herbs for the care of various medical problems. Taking herbs and supplements can be especially harmful to a person with thyroid disease as they may interfere with your medication and/or the functioning of your thyroid gland.
Chiropractors
According to the American Chiropractic Association, chiropractors are designated as “physician-level providers,” in the vast majority of states. While the doctor of chiropractic (DC) program is similar to the doctor of medicine (MD) program in the first two years, the programs diverge in the second half. During this time, the DC program focuses on diet, nutrition, and spinal manipulation, while the MD program emphasizes the study of pharmacology.5
Complement to Your Thyroid Care
While your chiropractor may have been the one to diagnose your thyroid disease (they can order laboratory tests and imaging studies, like a naturopath), once diagnosed, your chiropractor must refer you to a medical doctor for proper treatment—for instance, thyroid hormone replacement for hypothyroidism and either an anti-thyroid drug, surgery, or radioactive iodine ablation for hyperthyroidism.
Chiropractors can, however, provide supportive thyroid care, such as nutritional guidance or ways to ease musculoskeletal pain associated with the underlying thyroid disease (like carpal tunnel syndrome or joint aches).
Chiropractors are legally prohibited from prescribing thyroid medication, which means that they cannot treat or cure thyroid conditions.
A Word From Verywell
The decision to find a doctor for your thyroid care can be a challenging one, as the relationship is an intensely personal one, and it’s not easy to find the right match, particularly when you may be limited by geography and insurance.
Remain proactive in seeking out the right doctor-patient relationship. And keep a positive mindset, too. When you find that trusting, compassionate partnership, you will just know it.
Tests for Thyroid Cancer
This resources was originally published by the American Cancer Society here.
Thyroid cancer may be diagnosed after a person goes to a doctor because of symptoms, or it might be found during a routine physical exam or other tests. If there is a reason to suspect you might have thyroid cancer, your doctor will use one or more tests to confirm the diagnosis. If cancer is found, other tests might be done to find out more about the cancer.
Medical history and physical exam
If you have any signs or symptoms that suggest you might have thyroid cancer, your health care professional will want to know your complete medical history. You will be asked questions about your possible risk factors, symptoms, and any other health problems or concerns. If someone in your family has had thyroid cancer (especially medullary thyroid cancer) or tumors called pheochromocytomas, it is important to tell your doctor, as you might be at high risk for this disease.
Your doctor will examine you to get more information about possible signs of thyroid cancer and other health problems. During the exam, the doctor will pay special attention to the size and firmness of your thyroid and any enlarged lymph nodes in your neck.
Imaging tests
Imaging tests may be done for a number of reasons:
- To help find suspicious areas that might be cancer
- To learn how far cancer may have spread
- To help determine if treatment is working
People who have or may have thyroid cancer will get one or more of these tests.
Ultrasound
Ultrasound uses sound waves to create images of parts of your body. You are not exposed to radiation during this test.
This test can help determine if a thyroid nodule is solid or filled with fluid. (Solid nodules are more likely to be cancerous.) It can also be used to check the number and size of thyroid nodules as well as help determine if any nearby lymph nodes are enlarged because the thyroid cancer has spread.
For thyroid nodules that are too small to feel, this test can be used to guide a biopsy needle into the nodule to get a sample. Even when a nodule is large enough to feel, most doctors prefer to use ultrasound to guide the needle.
Radioiodine scan
Radioiodine scans can be used to help determine if someone with a lump in the neck might have thyroid cancer. They are also often used in people who have already been diagnosed with differentiated (papillary, follicular, or Hürthle cell) thyroid cancer to help show if it has spread. Because medullary thyroid cancer cells do not absorb iodine, radioiodine scans are not used for this cancer.
For this test, a small amount of radioactive iodine (called I-131) is swallowed (usually as a pill) or injected into a vein. Over time, the iodine is absorbed by the thyroid gland (or thyroid cells anywhere in the body). A special camera is used several hours later to see where the radioactivity is.
For a thyroid scan, the camera is placed in front of your neck to measure the amount of radiation in the gland. Abnormal areas of the thyroid that have less radioactivity than the surrounding tissue are called cold nodules, and areas that take up more radiation are called hot nodules. Hot nodules usually are not cancerous, but cold nodules can be benign or cancerous. Because both benign and cancerous nodules can appear cold, this test by itself can’t diagnose thyroid cancer.
After surgery for thyroid cancer, whole-body radioiodine scans are useful to look for possible spread throughout the body. These scans become even more sensitive if the entire thyroid gland has been removed by surgery because more of the radioactive iodine is picked up by any remaining thyroid cancer cells.
Radioiodine scans work best if patients have high blood levels of thyroid-stimulating hormone (TSH, or thyrotropin). For people whose thyroid has been removed, TSH levels can be increased by stopping thyroid hormone pills for a few weeks before the test. This leads to low thyroid hormone levels (hypothyroidism) and causes the pituitary gland to release more TSH, which in turn stimulates any thyroid cancer cells to take up the radioactive iodine. A downside of this is that it can cause the symptoms of hypothyroidism, including tiredness, depression, weight gain, sleepiness, constipation, muscle aches, and reduced concentration. One way to raise TSH levels without withholding thyroid hormone is to give an injectable form of thyrotropin (Thyrogen) before the scan.
Because any iodine already in the body can affect this test, people are usually told to avoid foods or medicines that contain iodine for a few days before the scan.
Radioactive iodine can also be used to treat differentiated thyroid cancer, but it is given in much higher doses. This type of treatment is described in Radioactive iodine (radioiodine) therapy.
Chest x-ray
If you have been diagnosed with thyroid cancer (especially follicular thyroid cancer), a plain x-ray of your chest may be done to see if cancer has spread to your lungs.
Computed tomography (CT) scan
The CT scan is an x-ray test that makes detailed cross-sectional images of your body. It can help determine the location and size of thyroid cancers and whether they have spread to nearby areas, although ultrasound is usually the test of choice. A CT scan can also be used to look for spread into distant organs such as the lungs.
One problem using CT scans is that the CT contrast dye contains iodine, which interferes with radioiodine scans. For this reason, many doctors prefer MRI scans for differentiated thyroid cancer.
Magnetic resonance imaging (MRI) scan
MRI scans use magnets instead of radiation to create detailed cross-sectional images of your body. MRI can be used to look for cancer in the thyroid, or cancer that has spread to nearby or distant parts of the body. But ultrasound is usually the first choice for looking at the thyroid. MRI can provide very detailed images of soft tissues such as the thyroid gland. MRI scans are also very helpful in looking at the brain and spinal cord.
Positron emission tomography (PET) scan
A PET scan can be very useful if your thyroid cancer is one that doesn’t take up radioactive iodine. In this situation, the PET scan may be able to tell whether the cancer has spread.
Biopsy
The actual diagnosis of thyroid cancer is made with a biopsy, in which cells from the suspicious area are removed and looked at in the lab.
If your doctor thinks a biopsy is needed, the simplest way to find out if a thyroid lump or nodule is cancerous is with a fine needle aspiration (FNA) of the thyroid nodule. This type of biopsy can sometimes be done in your doctor’s office or clinic.
Before the biopsy, local anesthesia (numbing medicine) may be injected into the skin over the nodule, but in most cases an anesthetic is not needed. Your doctor will place a thin, hollow needle directly into the nodule to aspirate (take out) some cells and a few drops of fluid into a syringe. The doctor usually repeats this 2 or 3 more times, taking samples from several areas of the nodule. The biopsy samples are then sent to a lab, where they are looked at to see if the cells look cancerous or benign.
Bleeding at the biopsy site is very rare except in people with bleeding disorders. Be sure to tell your doctor if you have problems with bleeding or are taking medicines that could affect bleeding, such as aspirin or blood thinners.
This test is generally done on all thyroid nodules that are big enough to be felt. This means that they are larger than about 1 centimeter (about 1/2 inch) across. Doctors often use ultrasound to see the thyroid during the biopsy, which helps make sure they are getting samples from the right areas. This is especially helpful for smaller nodules. FNA biopsies can also be used to get samples of swollen lymph nodes in the neck to see if they contain cancer.
Sometimes an FNA biopsy will need to be repeated because the samples didn’t contain enough cells. Most FNA biopsies will show that the thyroid nodule is benign. Rarely, the biopsy may come back as benign even though cancer is present. Cancer is clearly diagnosed in only about 1 of every 20 FNA biopsies.
Sometimes the test results first come back as “suspicious” or “of undetermined significance” if FNA findings don’t show for sure if the nodule is either benign or malignant. If this happens, the doctor may order lab tests on the sample (see below).
If the diagnosis is not clear after an FNA biopsy, you might need a more involved biopsy to get a better sample, particularly if the doctor has reason to think the nodule may be cancer. This might include a core biopsy using a larger needle, a surgical “open” biopsy to remove the nodule, or a lobectomy (removal of half of the thyroid gland). Surgical biopsies and lobectomies are done in an operating room while you are under general anesthesia (in a deep sleep). A lobectomy can also be the main treatment for some early cancers, although for many cancers the rest of the thyroid will need to be removed as well (during an operation called a completion thyroidectomy).
Lab tests of biopsy (or other) samples
In some cases, doctors might use molecular tests to look for specific gene changes in the cancer cells. This might be done for different reasons:
- If FNA biopsy results aren’t clear, the doctor might order lab tests on the samples to see if there are changes in the BRAF or RET/PTC genes. Finding one of these changes makes thyroid cancer much more likely.
- For some types of thyroid cancer, molecular tests might be done to see if the cancer cells have changes in certain genes (such as the BRAF, RET/PTC, or NTRK genes), which could mean that certain targeted drugs might be helpful in treating the cancer.
These tests can be done on tissue taken during a biopsy or surgery for thyroid cancer. If the biopsy sample is too small and all the molecular tests can’t be done, the testing may also be done on blood that is taken from a vein, just like a regular blood draw.
Blood tests
Blood tests are not used to find thyroid cancer. But they can help show if your thyroid is working normally, which may help the doctor decide what other tests may be needed. They can also be used to monitor certain cancers.
Thyroid-stimulating hormone (TSH)
Tests of blood levels of thyroid-stimulating hormone (TSH or thyrotropin) may be used to check the overall activity of your thyroid gland. Levels of TSH, which is made by the pituitary gland, may be high if the thyroid is not making enough hormones. This information can be used to help choose which imaging tests (such as ultrasound or radioiodine scans) to use to look at a thyroid nodule. The TSH level is usually normal in thyroid cancer.
T3 and T4 (thyroid hormones)
These are the main hormones made by the thyroid gland. Levels of these hormones may also be measured to get a sense of thyroid gland function. The T3 and T4 levels are usually normal in thyroid cancer.
Thyroglobulin
Thyroglobulin is a protein made by the thyroid gland. Measuring the thyroglobulin level in the blood can’t be used to diagnose thyroid cancer, but it can be helpful after treatment. A common way to treat thyroid cancer is to remove most of the thyroid by surgery and then use radioactive iodine to destroy any remaining thyroid cells. These treatments should lead to a very low level of thyroglobulin in the blood within several weeks. If it is not low, this might mean that there are still thyroid cancer cells in the body. If the level rises again after being low, it is a sign that the cancer could be coming back.
Calcitonin
Calcitonin is a hormone that helps control how the body uses calcium. It is made by C cells in the thyroid, the cells that can develop into medullary thyroid cancer (MTC). If MTC is suspected or if you have a family history of the disease, blood tests of calcitonin levels can help look for MTC. This test is also used to look for the possible recurrence of MTC after treatment. Because calcitonin can affect blood calcium levels, these may be checked as well.
Carcinoembryonic antigen (CEA)
People with MTC often have high blood levels of a protein called carcinoembryonic antigen (CEA). Tests for CEA can help monitor this cancer.
Other blood tests
You might have other blood tests as well. For example, if you are scheduled for surgery, tests will be done to check your blood cell counts, to look for bleeding disorders, and to check your liver and kidney function.
Medullary thyroid carcinoma (MTC) can be caused by a genetic syndrome that also causes a tumor called pheochromocytoma. Pheochromocytomas can cause problems during surgery if the patient is under anesthesia (in a deep sleep). This is why patients with MTC who will have surgery are often tested to see if they have a pheochromocytoma as well. This can mean blood tests for epinephrine (adrenaline) and a related hormone called norepinephrine, and/or urine tests for their breakdown products (called metanephrines).
Vocal cord exam (laryngoscopy)
Thyroid tumors can sometimes affect the vocal cords. If you are going to have surgery to treat thyroid cancer, a procedure called a laryngoscopy will probably be done first to see if the vocal cords are moving normally. For this exam, the doctor looks down the throat at the larynx (voice box) with special mirrors or with a laryngoscope, a thin tube with a light and a lens on the end for viewing.
Signs and Symptoms of Thyroid Cancer
This resources was originally published by the American Cancer Society here.
Thyroid cancer can cause any of the following signs or symptoms:
- A lump in the neck, sometimes growing quickly
- Swelling in the neck
- Pain in the front of the neck, sometimes going up to the ears
- Hoarseness or other voice changes that do not go away
- Trouble swallowing
- Trouble breathing
- A constant cough that is not due to a cold
If you have any of these signs or symptoms, talk to your doctor right away. Many of these symptoms can also be caused by non-cancerous conditions or even other cancers of the neck area. Lumps in the thyroid are common and are usually benign. Still, if you have any of these symptoms, it’s important to see your doctor so the cause can be found and treated, if needed.
What Is Thyroid Cancer?
This resources was originally published by the American Cancer Society here.
Thyroid cancer is a type of cancer that starts in the thyroid gland. Cancer starts when cells begin to grow out of control. (To learn more about how cancers start and spread, see What Is Cancer?)
The thyroid gland makes hormones that help regulate your metabolism, heart rate, blood pressure, and body temperature.
Where thyroid cancer starts
The thyroid gland is in the front part of the neck, below the thyroid cartilage (Adam’s apple). In most people, the thyroid cannot be seen or felt. It is shaped like a butterfly, with 2 lobes — the right lobe and the left lobe — joined by a narrow piece of gland called the isthmus (see picture below).
The thyroid gland has 2 main types of cells:
- Follicular cells use iodine from the blood to make thyroid hormones, which help regulate a person’s metabolism. Having too much thyroid hormone (hyperthyroidism) can cause a fast or irregular heartbeat, trouble sleeping, nervousness, hunger, weight loss, and a feeling of being too warm. Having too little hormone (hypothyroidism) causes a person to slow down, feel tired, and gain weight. The amount of thyroid hormone released by the thyroid is regulated by the pituitary gland at the base of the brain, which makes a substance called thyroid-stimulating hormone (TSH).
- C cells (also called parafollicular cells) make calcitonin, a hormone that helps control how the body uses calcium.
Other, less common cells in the thyroid gland include immune system cells (lymphocytes) and supportive (stromal) cells.
Different cancers develop from each kind of cell. The differences are important because they affect how serious the cancer is and what type of treatment is needed.
Many types of growths and tumors can develop in the thyroid gland. Most of these are benign (non-cancerous) but others are malignant (cancerous), which means they can spread into nearby tissues and to other parts of the body.
Benign thyroid conditions
Thyroid enlargement
Changes in the thyroid gland’s size and shape can often be felt or even seen by patients or by their doctor.
An abnormally large thyroid gland is sometimes called a goiter. Some goiters are diffuse, meaning that the whole gland is large. Other goiters are nodular, meaning that the gland is large and has one or more nodules (bumps) in it. There are many reasons the thyroid gland might be larger than usual, and most of the time it is not cancer. Both diffuse and nodular goiters are usually caused by an imbalance in certain hormones. For example, not getting enough iodine in the diet can cause changes in hormone levels and lead to a goiter.
Thyroid nodules
Lumps or bumps in the thyroid gland are called thyroid nodules. Most thyroid nodules are benign, but about 2 or 3 in 20 are cancerous. Sometimes these nodules make too much thyroid hormone and cause hyperthyroidism. Nodules that produce too much thyroid hormone are almost always benign.
People can develop thyroid nodules at any age, but they occur most commonly in older adults. Fewer than 1 in 10 adults have thyroid nodules that can be felt by a doctor. But when the thyroid is looked at with an ultrasound, many more people are found to have nodules that are too small to feel and most of them are benign.
Most nodules are cysts filled with fluid or with a stored form of thyroid hormone called colloid. Solid nodules have little fluid or colloid and are more likely to be cancerous. Still, most solid nodules are not cancer. Some types of solid nodules, such as hyperplastic nodules and adenomas, have too many cells, but the cells are not cancer cells.
Benign thyroid nodules sometimes can be left alone (not treated) and watched closely as long as they’re not growing or causing symptoms. Others may require some form of treatment.
Types of Thyroid Cancers
The main types of thyroid cancer are:
- Differentiated (including papillary, follicular and Hürthle cell)
- Medullary
- Anaplastic (an aggressive cancer)
Differentiated thyroid cancers
Most thyroid cancers are differentiated cancers. The cells in these cancers look a lot like normal thyroid tissue when seen in the lab. These cancers develop from thyroid follicular cells.
Papillary cancer (also called papillary carcinomas or papillary adenocarcinomas): About 8 out of 10 thyroid cancers are papillary cancers. These cancers tend to grow very slowly and usually develop in only one lobe of the thyroid gland. Even though they grow slowly, papillary cancers often spread to the lymph nodes in the neck. Even when these cancers have spread to the lymph nodes, they can often be treated successfully and are rarely fatal.
There are several subtypes of papillary cancers. Of these, the follicular subtype (also called mixed papillary-follicular variant) is most common. It has the same good outlook (prognosis) as the standard type of papillary cancer when found early, and they are treated the same way. Other subtypes of papillary carcinoma (columnar, tall cell, insular, and diffuse sclerosing) are not as common and tend to grow and spread more quickly.
Follicular cancer (also called follicular carcinoma or follicular adenocarcinoma): Follicular cancer is the next most common type, making up about 1 out of 10 thyroid cancers. It is more common in countries where people don’t get enough iodine in their diet. These cancers usually do not spread to lymph nodes, but they can spread to other parts of the body, such as the lungs or bones. The outlook (prognosis) for follicular cancer is not quite as good as that of papillary cancer, although it is still very good in most cases.
Hürthle (Hurthle) cell cancer (also called oxyphil cell carcinoma): About 3% of thyroid cancers are this type. It is harder to find and to treat.
Medullary thyroid carcinoma
Medullary thyroid cancer (MTC) accounts for about 4% of thyroid cancers. It develops from the C cells of the thyroid gland, which normally make calcitonin, a hormone that helps control the amount of calcium in blood. Sometimes this cancer can spread to lymph nodes, the lungs, or liver even before a thyroid nodule is discovered.
This type of thyroid cancer is more difficult to find and treat, There are 2 types of MTC:
- Sporadic MTC, which accounts for about 8 out of 10 cases of MTC, is not inherited (meaning it does not run in families). It occurs mostly in older adults and often affects only one thyroid lobe.
- Familial MTC is inherited and 20% to 25% can occur in each generation of a family. These cancers often develop during childhood or early adulthood and can spread early. Patients usually have cancer in several areas of both lobes. Familial MTC is often linked with an increased risk of other types of tumors. This is described in more detail in Thyroid Cancer Risk Factors.
Anaplastic (undifferentiated) thyroid cancer
Anaplastic carcinoma (also called undifferentiated carcinoma) is a rare form of thyroid cancer, making up about 2% of all thyroid cancers. It is thought to sometimes develop from an existing papillary or follicular cancer. This cancer is called undifferentiated because the cancer cells do not look very much like normal thyroid cells. This cancer often spreads quickly into the neck and to other parts of the body, and is very hard to treat.
Less Common Thyroid Cancers
Less than 4% of cancers found in the thyroid are thyroid lymphomas, thyroid sarcomas, or other rare tumors.
Parathyroid cancer
Behind, but attached to, the thyroid gland are 4 tiny glands called the parathyroids. The parathyroid glands help regulate the body’s calcium levels. Cancers of the parathyroid glands are very rare — there are probably fewer than 100 cases each year in the United States.
Parathyroid cancers are often found because they cause high blood calcium levels. This makes a person tired, weak, and drowsy. It can also make you urinate (pee) a lot, causing dehydration, which can make the weakness and drowsiness worse. Other symptoms include bone pain and fractures, pain from kidney stones, depression, and constipation.
Larger parathyroid cancers may also be found as a nodule near the thyroid. No matter how large the nodule is, the only treatment is to remove it surgically. Parathyroid cancer is much harder to cure than thyroid cancer.
Top Resources for Thyroid Cancer
General Resources, Including Medical Information
- thyca.org– Thyca, Inc. (has everything you need to know about thyroid cancer as well as general thyroid information)
- cancer.gov– National Cancer Institute
- aacr.org– American Association for Cancer Research
- asco.org– American Society of Clinical Oncology
- cancer.org– American Cancer Society
- thyroid.org– American Thyroid Association
- clinicaltrials.gov– Find a clinical trial
- nccn.org– National Comprehensive Cancer Network
- oncolink.org– University of Pennsylvania’s Abraham Cancer Center
- cancer.net
- cancercare.org
- nord.org- National Organization of Rare Diseases
- triagecancer.org
- cancerquest.org
- thyroidawareness.com
- thancguide.org – The Thyroid, Head and Neck Cancer (THANC) Foundation
- thepatientstory.com/cancers/thyroid – Patient stories
Find a Physician
- healthgrades.com
- zocdoc.com
- American Thyroid Association – find an endocrinologist
- American Association of Clinical Endocrinologists – find an endocrinologist
- The American Association of Endocrine Surgeons – find an endocrinologist
Support Groups
- Many support groups can be found on Facebook by type of cancer and/or variant
- Thyca
- Our Odyssey– for young adults
- Inspire
- CancerCare
- Immerman Angels
- Lacuna Loft– for young adults
- Stupid Cancer– for young adults
- Cancer Support Community
Carly Flumer is a young woman who was diagnosed with stage I papillary thyroid cancer at the age of 27. She recently received her Master’s degree from Boston University in Health Communication and received her Bachelor’s from George Mason University in Health Administration and Policy. While being diagnosed with the “C” word at such a young age was a surprise, as it would be to anyone, she found strength, support, and inspiration in sharing her cancer journey on social media. As a result of her health outcome, she looks to advocate for other cancer patients through education, research, and health literacy.
Thyroid Cancer Glossary of Terms
Thyroid Conditions
Hyperthyroidism – A condition that occurs when the thyroid gland makes more thyroid hormones than the body needs. Thyroid hormones control the way the body uses energy and affect the body’s metabolism. Signs and symptoms include weight loss, fatigue, rapid or irregular heartbeat, sweating, diarrhea, nervousness, mood swings, shaky hands, trouble sleeping, trouble tolerating heat, muscle weakness, and a goiter (an enlarged thyroid gland that may cause the bottom of the neck to look swollen). Also called overactive thyroid.
Hypothyroidism – Too little thyroid hormone. Symptoms include weight gain, constipation, dry skin, and sensitivity to the cold. Also called under active thyroid
Types of Thyroid Cancer
Anaplastic Thyroid Cancer – a rare, aggressive type of thyroid cancer in which the malignant (cancer) cells look very different from normal thyroid cells
Follicular Thyroid Cancer – cancer that forms in follicular cells in the thyroid. It grows slowly and is highly treatable. The cancer cells look and act in some respects like normal thyroid cells
Medullary Thyroid Cancer – cancer that develops in C cells of the thyroid. The C cells make a hormone (calcitonin) that helps maintain a healthy level of calcium in the blood
Papillary Thyroid Cancer – cancer that forms in follicular cells in the thyroid and grows in small finger-like shapes. It is the most common type of thyroid cancer. The cancer cells look and act in some respects like normal thyroid cells. Variants include:
- Columnar cell
- Cribiform-Morular
- Diffuse sclerosing
- Encapsulated
- Follicular variant of papillary
- Hobnail
- Hürthle cell
- Insular
- Macrofollicular
- Oncocytic
- Solid/trabecular
- Spindle cell
- Tall cell
- Warthin-Like
Poorly Differentiated Thyroid Cancer – a rare form of thyroid cancer that is often aggressive. It is associated with high risk of cancer recurrence, spread to lung and/or bones and increased risk of death. Patients are often treated with a combination of surgery, radioactive iodine and/or radiation therapy and possibly newer, molecular targeted therapies
Thyroid Cancer Terms to Know
Adenocarcinoma – Cancer that begins in glandular cells. Glandular cells are found in tissue that lines certain internal organs and makes and releases substances in the body, such as mucus, digestive juices, or other fluids
Advanced – Has spread to other places in the body; far along in course
Benign – Not cancerous. Benign tumors may grow larger but do not spread to other parts of the body. Also called non-malignant
Lobe – a portion of an organ (ex. thyroid)
Lobectomy – surgery to remove a whole lobe (section) of an organ (ex. thyroid)
Locally Advanced – has spread to nearby tissues or lymph nodes
Malignant – Cancerous. Malignant cells can invade and destroy nearby tissue and spread to other parts of the body
Metastatic – spread of cancer from the primary site (place where it started) to other places in the body
Neoplasm – An abnormal mass of tissue that results when cells divide more than they should or do not die when they should. Neoplasms may be benign (not cancer), or malignant (cancer). Also called tumor
Nodule – A growth or lump that may be malignant (cancer) or benign (not cancer)
Partial Lobectomy – surgery to remove a whole organ (ex. thyroid)
Radioactive Iodine – a radioactive form of iodine, often used for imaging tests or to treat an overactive thyroid, thyroid cancer, and certain other cancers. For imaging tests, the patient takes a small dose of radioactive iodine that collects in thyroid cells and certain kinds of tumors and can be detected by a scanner. To treat thyroid cancer, the patient takes a large dose of radioactive iodine, which kills thyroid cells. Radioactive iodine is given by mouth as a liquid or in capsules, by infusion, or sealed in seeds, which are placed in or near the tumor to kill cancer cells
Recurrent – Cancer that has recurred (come back), usually after a period of time during which the cancer could not be detected. The cancer may come back to the same place as the original (primary) tumor or to another place in the body. Also called recurrence and relapse
Refractory – Cancer that does not respond to treatment. The cancer may be resistant at the beginning of treatment or it may become resistant during treatment. Also called resistant cancer
Risk – patients with differentiated thyroid cancer (papillary or follicular) have different levels of risk of a recurrence or of persistent disease
- Low Risk of recurrence or persistent disease means: no cancer in nearby tissue or outside the thyroid bed other than 5 or fewer small involved lymph nodes (under 0.2 centimeters), and cancer that is not one of the variants.
- Intermediate Risk (Medium Risk) means some tumor in nearby neck tissue at the time of surgery, more than 5 lymph node metastases 0.2 to 3 centimeters in size, or a tumor that’s a variant or has vascular invasion
- High Risk means extensive tumor outside the thyroid, distant metastases, incomplete tumor removal, or a cancerous lymph node over 3 centimeters in size.
T3 – also called triiodothyronine; a type of thyroid hormone
T4 – also called thyroxin and thyroxine; a hormone that is made by the thyroid gland and contains iodine. T4 increases the rate of chemical reactions in cells and helps control growth and development. T4 can also be made in the laboratory and is used to treat thyroid disorders
Thyroglobulin – the form that thyroid hormone takes when stored in the cells of the thyroid. Doctors measure thyroglobulin level in blood to detect thyroid cancer cells that remain in the body after treatment. If the thyroid has been removed, thyroglobulin should not show up on a blood test. Some patients produce anti-thyroglobulin antibodies, which are not harmful but which mask the reliability of the thyroglobulin value
Thyroid Gland – a gland located beneath the larynx (voice box) that makes thyroid hormone and calcitonin. The thyroid helps regulate growth and metabolism. Also called thyroid gland
Thyroid Gland Squamous Cell Carcinoma – A rapidly growing primary carcinoma of the thyroid gland composed of malignant squamous cells (cells are found in the tissues that form the surface of the skin, the passages of the respiratory and digestive tracts, and the lining of the hollow organs of the body). The clinical course is usually aggressive
Stage – The extent of a cancer in the body. Staging is usually based on the size of the tumor, whether lymph nodes contain cancer, and whether the cancer has spread from the original site to other parts of the body
Unresectable – Unable to be removed with surgery
Sources:
cancer.gov
Carly Flumer is a young woman who was diagnosed with stage I papillary thyroid cancer at the age of 27. She recently received her Master’s degree from Boston University in Health Communication and received her Bachelor’s from George Mason University in Health Administration and Policy. While being diagnosed with the “C” word at such a young age was a surprise, as it would be to anyone, she found strength, support, and inspiration in sharing her cancer journey on social media. As a result of her health outcome, she looks to advocate for other cancer patients through education, research, and health literacy.
