Acute myeloid leukemia (AML) is a fast-growing form of cancer of the blood and bone marrow. AML is the most common type of acute leukemia and occurs when the bone marrow begins to make blasts, cells that have not yet completely matured. These blasts normally develop into white blood cells, but AML, these cells do not develop and are unable to ward off infections.
In AML, the bone marrow may also make abnormal red blood cells and platelets. The number of these abnormal cells increases rapidly, and the abnormal cells begin to crowd out the normal white blood cells, red blood cells and platelets that the body needs.
When people are anxious about their diagnosis, I think the best thing to do is to keep an eye on the bigger picture. I know your life is going to change. We can’t even make plans more than one week ahead of time. So, it’s important to keep an eye on the bigger picture. And the bigger picture is this is a steppingstone in your journey. This is a place, a situation, that you’re placed in that you’re having to undergo. But overall, you have a life outside of AML. You’ve had a life outside of AML. And keeping that bigger picture in the back of your head is very important. It’s very sane. You had a life. You enjoyed things before. You enjoyed going to the movies. You enjoy having dinners with your friends. You enjoy reading books. And so, it’s very healthy to continue to do those things and not get so consumed by the AML diagnosis and what is going on.
It will affect your life and it’s very important to keep doing what you’re doing. If you exercise, continue exercising. If you enjoy going to the movies, continue going to the movies with the expectation that you may not do that all of the time as you did before but you, certainly, can continue to do that because it keeps your head clear. It keeps you human because so much of AML takes away from you and you feel like you’re this thing, you’re this number. You’re the medical record number. You are Mr. so and so or you are a diagnosis. You are an AML diagnosis. It keeps you human to keep an eye on the bigger picture.
https://powerfulpatients.org/wp-content/uploads/Overcoming-Anxiety.png600600Caitlin McDonaldhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngCaitlin McDonald2019-06-27 18:57:412022-10-25 13:16:17Overcoming the Anxiety of an AML Diagnosis
Mayra Lee, a Registered Nurse, explains the positive benefits of educating yourself about AML and outlines key steps for learning more about your disease. Download the Find Your Voice Resource Guide here.
Mayra Lee, RN, is an outpatient clinic nurse at Moffitt Cancer Center. More about the expert.
So, the benefit of becoming informed about your disease when you’re diagnosed with AML would be that you are empowered. You will be empowered to – so much control is lost when you hear the word cancer. So much of your life changes in a matter of days or weeks from the time you’re told you have AML. Becoming informed about the treatments, about your disease, about what it is, about what the next step is empowers you to have control of the disease again when so much of your life is going to be out of control. It makes you be the driver in the disease along with your medical team. The medical team will steer you in which direction we think we should go but you will, ultimately, be the one making the decision with your team. You will not feel like the decision was made by your doctor. The decision is made together as it should be. The patient, the family, and the physicians and the team of medical people that take care of you.
It will not be something that your doctor does alone or that you’re doing alone because this is a very long journey, a very tedious journey. And the more you know about it also the less scared and the less stressed out you are about the diagnosis itself.
Patients can take key steps such as to become informed about their disease such as I think the first step would be to pick up those informational books or educational books that you will see out in the lobby in most physicians’ offices about AML, what is AML. That is step No. 1. Asking the nurses and the doctors do you have any information on my diagnosis, is there a reputable website that you recommend. There is a lot out there on the internet but a lot is not reputable and a lot is just hearsay.
And a lot of it is patients sharing in their own stories, which are all good formats but in the very beginning, you want to go to reputable websites. You want to hear it from NCCN or any one of those websites that have really good information about what the disease really is. And then, you can navigate whichever way you want, if you want to join those forums. And then, you’re better informed and you’re better educated as to what to expect.
https://powerfulpatients.org/wp-content/uploads/AML-Educated.png600600Caitlin McDonaldhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngCaitlin McDonald2019-06-21 18:54:552022-10-25 13:16:17Why Should You Become Educated about Your AML?
Last week, we hosted an Empowered #patientchat on leveraging social media for patient advocacy. The #patientchat community came together for an engaging discussion and shared their best advice and tips.
Top Tweets and Advice
Care Coordination Means Everyone Is Working Together
You Are Your Own Best Advocate
Work For What You Deserve
Full Chat
https://powerfulpatients.org/wp-content/uploads/Leveraging-Social-Media-for-Patient-Advocacy-patientchat-Highlights-1.png600600Caitlin McDonaldhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngCaitlin McDonald2019-06-21 18:17:152022-02-16 15:49:51How Does An Empowered Patient Approach Care Coordination? #patientchat Highlights
Brittany DeGreef, a genetic counselor, explains the difference between hereditary genetic testing for cancer risk and genetic testing following a cancer diagnosis.
Brittany DeGreef is a Genetic Counselor at Robert H. Lurie Comprehensive Cancer Center of Northwestern University. More about this expert.
My name is Brittany DeGreef and I am a licensed and certified genetic counselor and I work primarily in oncology genetics. At the Lurie Cancer Center, what I do is I provide comprehensive genetic counseling services for patients and families. Basically, what I do is take in family and personal history.
I help interpret what patterns we’re seeing in families. I provide risk assessment. Then we order and interpret genetic testing results. Based on those results, sometimes we make medical management recommendations for patients and families within a multi-disciplinary team within oncology at Northwestern.
The difference between predictive genetic testing and cancer genetic testing – let’s start with predictive genetic testing first. This means that we are testing someone who might be at risk for a specific hereditary condition, in particular, hereditary cancer syndromes.
In this case, what we’re doing is testing someone who is asymptomatic or does not have any signs of cancer at this point. What we’re trying to do is to identify if that person might be at high risk for specific cancers and implement certain screening strategies to risk reduction procedures and implement surveillance, if needed, if someone is at high risk for specific cancers.
When we think of cancer genetic testing, this person is likely already diagnosed with cancer and what we’re doing is trying to figure out if this person inherited something from either their mom or dad that placed them at a higher risk to get cancer in the first place.
In the past, this type of testing did not impact treatment strategies. But recently, this has been kind of the forefront of medicine where we are seeing patients who are just diagnosed with cancer and they are using genetic testing information to then incorporate that into their treatment approach.
https://powerfulpatients.org/wp-content/uploads/AML-Family.png600600Caitlin McDonaldhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngCaitlin McDonald2019-06-19 18:44:022022-10-25 13:16:17Predictive (Familial) Genetic Testing vs. Cancer Genetic Testing: What’s the Difference?
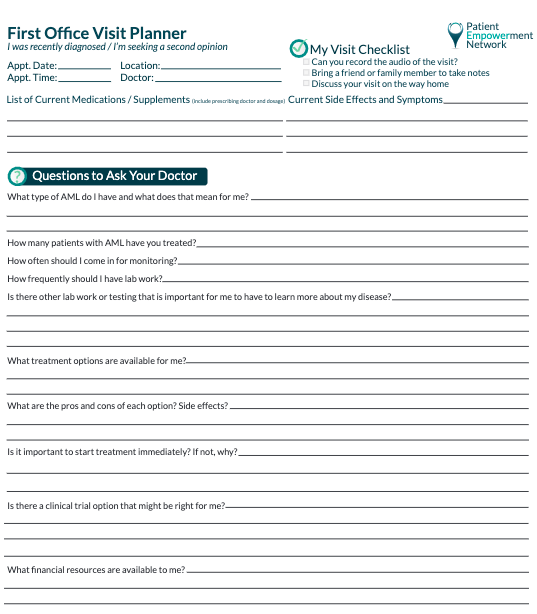
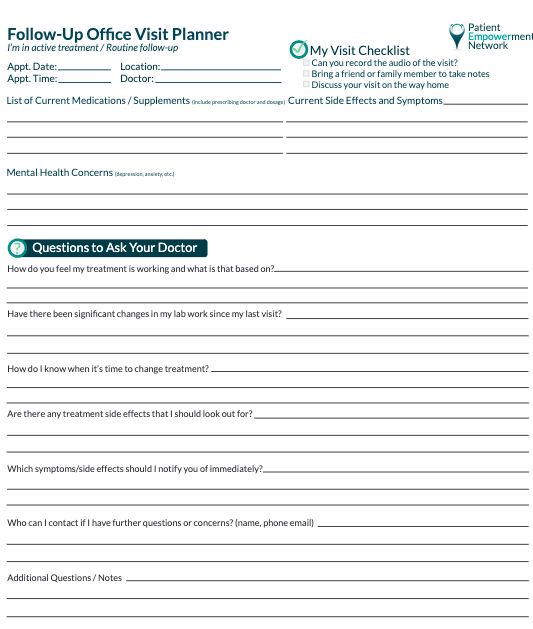
Registered nurse, Mayra Lee, outlines essential steps for making the most of appointments with your AML team. Download the Office Visit Planner and bring it to your next appointment here.
Mayra Lee, RN, is an outpatient clinic nurse at Moffitt Cancer Center. More about the expert.
During an initial visit, patients often forget to ask about how the treatment for their AML cancer is going to impact the quality of their life and all of the things that they do on a daily basis and being impacted by such a treatment. Treatments are, often times, discussed about we’re going to do X chemo or Y chemo, seven plus three, three plus seven, five days on Dacogen, whatever it may be. But the patients don’t often grasp the amount of quality of life that will be taken from their lives.
Other things that impact the quality of their life is a financial burden that the treatments bring about, having caretakers around them. We often see patients that don’t have a lot of family members or don’t have family here in the state that they’re residing in and they don’t have a lot of support. So, these are all things that are going to be impacted by the treatments for AML. And a lot of times, patients don’t ask that question very clearly about what is the realistic expectations of my life during the treatment phase.
Patients can best prepare for an office visit by asking questions, writing down the questions, before they come to the office and having it prepared.
And I think it’s very important for patients to write those questions down before they come to their treatment. It’s also very important to bring a note pad and a pen and write down things that are being said during your visit, whether it be the first time you hear this or a second or third opinion is very important to write down treatments. It’s important to write down things that you might not have picked up on the first visit when you were first diagnosed like chromosomes and different treatments and different tests that are going to be ordered. It’ very difficult to retain all of that information in one sitting. So, it’s important to bring a note pad and bring a friend to write those things down with you.
It’s very important to bring a family member or a friend to your appointments because that person – you can bounce back ideas and you can bounce back information.
You’re not there alone and it makes you feel like you’re not carrying the burden of now distributing this information to your friends and your family who are, obviously, very worried about you, your prognosis, your diagnosis, what did the doctor say. And you have someone else to say oh, they said this or the doctor said that. And you will not remember everything that was said in one sitting. So, bringing your friend or family member helps put all of that information together and helps recall everything that was said in that visit.
https://powerfulpatients.org/wp-content/uploads/AML-Team.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-17 19:08:432022-11-08 14:22:56Optimize Your First Visit with Your AML Team
Dr. Elizabeth Bowhay-Carnes provides advice on key genetic tests that should take place after an AML diagnosis and how they can inform your treatment options. Download the Find Your Voice Resource Guide here.
Dr. Elizabeth Bowhay–Carnes is Director of the Adult Non-Malignant Hematology Program and Co-Director of the Adolescent/Young Adult Oncology Program at Mays Cancer Center, home to UT Health San Antonio MD Anderson Cancer Center. More about this expert.
When a patient is first diagnosed with AML, or Acute Myeloid Leukemia, that test comes back initially as a test called flow cytometry, and that is really just one of the very first initial tests that is needed in the workup.
AML does not have traditional staging, as solid tumors have. There’s no such thing as a stage one, two, three, four. Instead, AML is divided into different risk categories. We call those low-risk, intermediate-risk, or high-risk, or sometimes we use the term standard-risk, intermediate-risk, high-risk.
And that information is determined from some specialty tests that we call cytogenetics. Sometimes we use the term molecular testing or next-generation sequencing. Those three different terms, cytogenetics, molecular, next generation sequencing, are all specialty lab tests that help us determine what risk category group does a patient fall in.
So, when a patient is first diagnosed with AML, that is very important to establish the initial diagnosis, but there’s those important follow-up tests that are done over the following weeks of treatment, from diagnosis at the beginning of treatment, that determine what a patient’s risk categories are. That information is very important because when we talk about initial treatment, a lot of the time that initial treatment is the same for all patients.
But then, there are other medications that can be added on, or different steps in the treatment process, that vary based on a patient’s individual risk category and risk characteristic.
https://powerfulpatients.org/wp-content/uploads/genetic-testing-1.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-12 16:49:332022-10-25 13:16:17Key Genetic Testing after an AML Diagnosis
Dr. Elizabeth Bowhay-Carnes provides advice for patients facing an AML diagnosis, including the necessity of putting together a strong healthcare team and leaning on your personal support system. Download the Find Your Voice Resource Guide here.
Dr. Elizabeth Bowhay–Carnes is Director of the Adult Non-Malignant Hematology Program and Co-Director of the Adolescent/Young Adult Oncology Program at Mays Cancer Center, home to UT Health San Antonio MD Anderson Cancer Center. More about this expert.
My name is Dr. Elizabeth Bowhay-Carnes. I work at UT Health San Antonio MD Anderson Cancer Center, and I am a blood specialist. I specialize in taking care of patients that have various blood disorders, and my passion is working with patients and their families when someone is diagnosed with a blood cancer.
If I was a patient who was diagnosed with AML today, the first thing I would want to do is take a deep breath. When somebody is diagnosed with AML, this is a disorder that comes on suddenly, and so usually a patient and family are in shock. Usually, somebody was perfectly healthy a couple weeks before their presentation and then they find themselves admitted in a hospital, or a hospital setting, feeling quite ill. And so, one of the first things I would do is to make sure I understand who my care team will be. Fighting cancer is a team sport.
It is not an individual event. Although the patient is the most valuable player, there’s different parts of the team that are needed to get somebody through this diagnosis and their treatment. If I was the patient, I would make sure I understood who would be in charge of my treatment plan or who would be the attending physician. I would want to know who the main nursing contact or support person would be. If there’s calls in the middle of the night or emergencies, who’s the first person to call? I would want to make sure I have a family or friend support person designated as the main supportive role, who would help me fight through this process. Again, if I was diagnosed with AML today, I would take a deep breath, and I would re-center myself and establish who my care team would be.
https://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.png00Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-12 16:44:122022-10-25 13:16:16What Would You Do? AML Advice From An Expert
Brittany DeGreef, a genetic counselor, provides essential advice for when you are facing a cancer diagnosis emphasizing that leaning on supportive friends and family is key. Download the Office Visit Planner and bring it to your next appointment here.
Brittany Degreef is a Genetic Counselor at Robert H. Lurie Comprehensive Cancer Center of Northwestern University. More about this expert.
One piece of advice I give patients who are just diagnosed with cancer – and we do frequently see patients at least once a week who were just diagnosed either that week or the week prior – is feel what you need to feel. Not every patient is going to react or cope with their diagnosis in the same way as someone next to them, even within the same family. That also goes for caregivers and relatives.
So, just because you feel like helping out a relative in a specific way, it might not be the same for your brother or sister or cousin.
So, we always tell patients that there is no wrong or right way to cope with a diagnosis of cancer. The way that you approach it is perfectly fine and there’s no right or wrong way to do that.
So, another piece of advice we always tell patients is don’t be scared to lean on your support network, whether that be family or friends, your healthcare provider, advocacy groups, never be afraid to ask for help.
And for some patients who feel like they have limited resources, usually hospitals where you’re receiving your patient care has many resources available to you, whether that be emotional, financial, spiritual, logistical. Don’t be scared to ask about those resources.
https://powerfulpatients.org/wp-content/uploads/advice.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-12 16:22:532022-10-25 13:16:16Facing a Cancer Diagnosis: Advice From An Expert
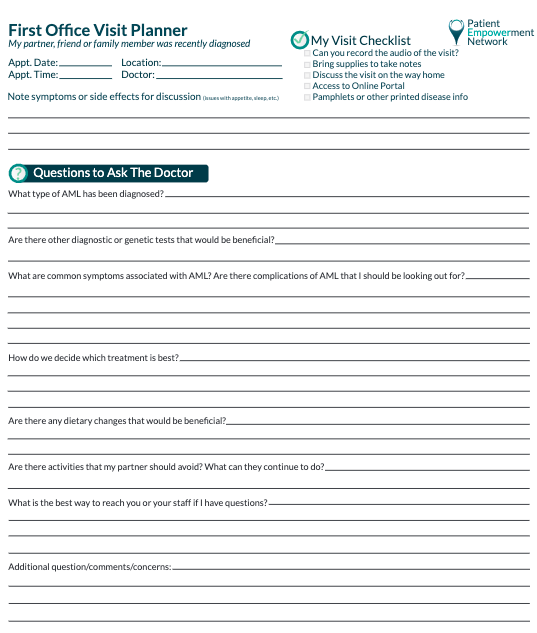
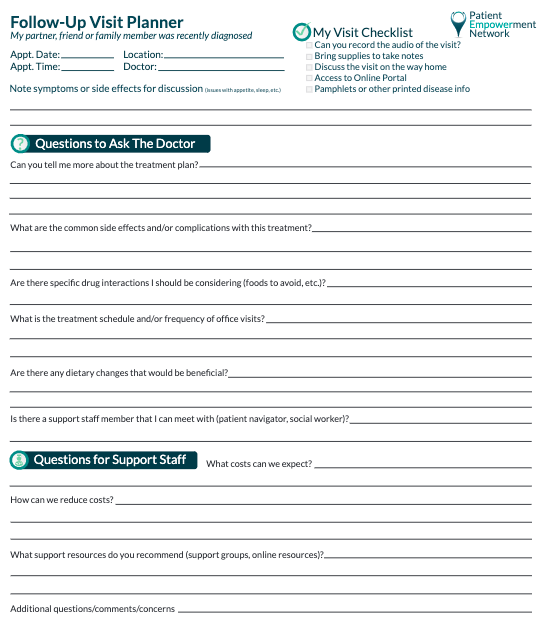
Appointments with your physician can be overwhelming. To optimize your visit, it’s best to arrive organized and prepared to take notes. Our Office Visit Planner can help. Guides for your first office visit as well as your follow-up office visit, tailored for patients and caregivers, are available below. Download, print and bring along with you to the appointment.
In the spring of 2016, I was looking forward to a final year of teaching sociology before a retirement promising new adventures. I felt great and had no reason to think I had any health problems. When my doctor suggested some routine blood work, I readily complied. When the results showed abnormally low white blood cell counts and he recommended a hematologist, I readily complied. When the hematologist ordered a bone marrow biopsy, I still readily complied. When the results came in, my life changed forever.
The biopsy revealed that I had acute myeloid leukemia. Since this disease can kill within months, they recommended immediate treatment. The next day I checked into a hospital and started chemotherapy. I received the standard treatment for this disease for the preceding 40 years: a “7 + 3” cocktail of cytarabine and idarubicin. I spent five and a half weeks in the hospital dealing with various infections brought on by immunosuppression and patiently waiting for my blood counts to recover. As they did, I received the best possible news. The chemotherapy had achieved a temporary remission that bought me time to explore my options for longer term treatment.
As I awaited the molecular and cytogenic data on my cancer, I was told to expect two possibilities. If there was a relatively low risk of relapse, I might get by with additional chemotherapy. If there was a high risk of relapse, a stem cell transplant was in order. When the results placed me in an intermediate risk category, I had a tough choice to make. After researching my options, getting second opinions, gathering advice, and reading my doctor’s cues, I settled on the transplant. My logic was that if I opted for more chemo and it didn’t work out, I would deeply regret not having the transplant. If I had the transplant and it didn’t work out, at least I would feel as if I gave it my best shot and it just wasn’t meant to be. Despite the 15-20% mortality rate from the transplant itself, I was at peace with my decision to proceed.
My benefactors were two anonymous sets of parents who had donated their newborn infants’ umbilical cords to a transplant bank. Once we found two good matches, the cords were shipped to my transplant hospital, the cord blood was extracted, and it was transfused into my bloodstream. These stem cells just “knew” where to go to engraft in my bone marrow and begin producing a healthy new immune system. For the second time, I received the best possible news. Three weeks after transplant, one of my donor’s cells were 99% engrafted. With that result, I returned home for a prolonged recovery.
For the next few weeks, I faced daily clinic visits, blood tests, transfusions of platelets and red blood cells, growth factor injections, and lingering effects of my conditioning chemotherapy and radiation as well as the engraftment process itself. As the weeks turned into months, my recovery proceeded apace. It eventually became clear that I could claim the best possible news for the third time, as my new cells and old body got along with each other and there was no evidence of graft-vs.-host disease. Looking back over the entire process, my oncologist summarized it by saying “this is as good as it gets.”
Many people wanted to give me credit for surviving this disease. While it is tempting to claim such credit, I remain agnostic about whether anything I did had a material effect on my positive outcome. I think my survival was largely a matter of luck, chance, and random variation across AML patients. Nonetheless, there were several practices I engaged in throughout my treatment that deserve mention. At the very least, they brought me peace during a difficult time. And at the most, they may indeed have contributed to a positive outcome for which I am eternally grateful.
The first set of practices that sustained me was mindfulness, meditation and yoga. To the greatest extent possible, these practices helped me let go of ruminations about the past or fears about the future and focus on the present moment. Focusing on my breathing kept me centered as – like my breaths – each moment flowed into the next. Maintaining a non-judgmental awareness and acceptance of each passing moment kept my psyche on an even keel.
Rather than extended periods of formal meditation, I simply sought a mindful awareness of each moment, hour, day and week. I also went through a daily yoga routine even while receiving chemotherapy. Doing so helped me retain my identity as I weathered the toxic treatment and its inevitable side-effects. In the evenings, I used a technique called a body scan to relax and prepare me for a peaceful sleep. The cumulative effect of these practices was a calm acceptance of circumstances I could not change alongside a serene hope that all would work out for the best.
A second practice involved being a proactive patient. Perhaps it was my training as a social scientist that allowed me to bring an analytical curiosity to my disease and the treatments my doctors were deploying. I asked lots of questions during their all too brief visits, and they patiently responded to all my queries.
On several occasions, my proactive stance made a positive contribution to my treatment. When I developed a nasty, full body rash, it took a collaborative conversation between me, my oncologist, and infectious disease doctors to isolate the one drug among so many that was the culprit. I identified it, they switched it out, and the rash abated. On another occasion, I was able to identify two drugs that were causing an unpleasant interaction effect. I suggested changing the dosing schedule, they concurred, and the problem resolved. The sense of efficacy I received from this proactive stance also helped me retain a positive mood and hopeful stance during my prolonged treatment.
A third practice involved maintaining a regimen of physical activity. During my first, five-week hospital stay, I felt compelled to move and get out of my room for both physical and social reasons. I developed a routine of walking the halls three times a day, trailing my IV pole behind me. They tell me I was walking roughly 5 miles a day, and every excursion felt like it was keeping my disease at bay and connecting me with all the nurses and staff members I would encounter as I made my rounds.
When I moved to my transplant hospital, I was confined to my room but requested a treadmill that met the physical need for activity even as I sacrificed the social benefits of roaming the halls. But throughout both hospital stays and later at home, I maintained stretching activities, exercise workouts, physical therapy routines, and yoga to keep my body as active and engaged as my circumstances would allow. These activities also gave me a welcome sense of efficacy and control.
A fourth practice involved maintaining my sense of humor. I have always appreciated a wide variety of humor, ranging from bad jokes, puns and double entendre to witty anecdotes and stories to philosophical musings. Cancer is anything buy funny, which is precisely why humor has the power to break through the somber mood and fatalistic worldview that so often accompanies the disease. Using humor became another way of keeping the cancer at bay. It was a way of saying you may make me sick and eventually kill me, but I’m still going to enjoy a good laugh and a bad joke along the way.
Alongside these practices I could control, there were also beneficial circumstances beyond my control that worked in my favor. These included the privilege of being a well-educated white male that led to my being treated respectfully and taken seriously by all my health care providers. In addition, my doctors and nurses consistently combined skill and expertise with compassion and empathy in ways I will never forget or could ever repay. And finally, my privileged status and excellent care played out against a backdrop of strong social support from a dense network of family, friends, colleagues and neighbors.
A final practice that integrated everything else was writing my story as it unfolded. Upon my first hospitalization, I began sending emails to an ever-expanding group of recipients documenting and reflecting upon my disease, treatment and recovery. Narrating my story for others required me to make sense of it for myself. The ostensible goal of keeping others informed became a powerful therapeutic prod for my own understanding of what was going on around me and to me. While my doctors’ ministrations cured my body, my writing preserved my sense of self and a coherent identity.
I eventually sent over 60 lengthy reports to a group of roughly 50 recipients over a 16-month period. This writing would eventually serve three purposes. It was a sense-making procedure for me. It was a communication vehicle with my correspondents. And finally, I realized it could be a resource for others in the broader cancer community. With that insight, I did some additional writing about lessons learned and identity transformations and published the resulting account.
As I mentioned at the start, I will never know if any of these practices or circumstances made a material contribution to my survival. But they maintained my sanity and preserved my identity during the most challenging experience of my life. Regardless of the eventual endings of our journeys, sustaining and nurturing ourselves along the way is a worthy goal in itself.
Steve Buechler is the author of “How Steve Became Ralph: A Cancer/Stem Cell Odyssey (with Jokes),” which was recently selected as an inspirational “Suggested Reading” by the Leukemia and Lymphoma Society. He recently recorded a 5-part webcast series that expands on his recovery story here. Steve’s numerous blog posts, video presentations, and more may be found at www.stevebuechlerauthor.com and he is on Facebook at SteveBuechlerAuthor.
https://powerfulpatients.org/wp-content/uploads/Facing-Acute-Myeloid-Leukemia_-Notes-from-a-Survivor”.png600600Steve Buechlerhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngSteve Buechler2019-06-11 16:49:272024-01-24 14:07:41Facing Acute Myeloid Leukemia: Notes from a Survivor
Every year over 525,000 Americans experiences their first heart attack while around 795,000 people experience strokes. Of that number, 75 percent of them are aged 65 and over. Recovering from medical conditions such as these can be a long road for older people. As we age, so does our bodies and immune system and recovery can take a longer time. The process of healing and returning to optimal health can be a stressful and trying time for both seniors and their caregivers, whether they are patients that are newly diagnosed or living with it for years. By implementing simple changes, you can ensure the process is a smooth and easy one for either yourself or a loved one.
Arrange For Help Sooner Rather Than Later – Both Personal And Infrastructural
The days immediately after medical events such as strokes, cardiac episodes, and even falls can find older Americans feeling frail and with limited movement. Small adjustments to both their living environment and making help available can help them in those initial times. Standard additions such as the placement of bath rails and reorganization of items to a more accessible level can help them maintain some level of independence and prevent further harm. Slips and falls are one of the most commonly reported incidents amongst seniors in America. Around1 in 4 older Americans experience falls each year and in those times where they are in long term recovery, these chances increase sizably.
In addition to making your home accessible, be sure to plan with other family members or carers a timetable to be present and help, particularly in the early days after being released from the hospital or care facilities. This is also the point where you will need to consider whether you can provide the level of long term care that person may need and do so comfortably at home.
Weigh Their Rehabilitation Options- Care Facilities Vs Recovering At Home
Speaking of providing long term care, considering the best rehabilitation option is one of the most important decisions in the recovery process of an older loved one. While most of us prefer to age at home, in a place surrounded by family and comfort there are cases where care facilities may prove to be better medically and financially. Some stroke patients can suffer long term loss of their motor skills and require round the clock care and physical rehabilitation. This can prove to be along, tough road and requires much commitment from both the caregivers and the patient. One of the most cited reasons for families not choosing assisted living is its costs. Take the time to inquire whether their state health insurance covers senior facilities and the extent of its coverage. Only then can you align your budgetary reach and make a decision on what you can afford.
Don’t Forget Their Mental Health
Our physical and mental health are strongly linked; a decline in one can impact the other. In long term recovery for seniors, this is particularly prevalent. Approximately 15 percent of adults 60 and older deal with mental illness including clinical depression. According to the Center For Disease Control and Prevention, 1-5 percent of the senior population are affected by depression. This can be further broken down into 13.5 percent of those that require home healthcare and 11.5 percent of those in hospitals. In addition, certain illnesses can trigger or worsen these symptoms including dementia, strokes and multiple sclerosis.
For those recovering, this can stem from long hospital stays or even PTSD from the actual event such as a stroke or fall. In long term recovery, there can also be a loss of motivation and sometimes, poor mental health can be influenced by a drastic change in their lifestyle such as regularly being active outdoors. It is important that we pay attention to both mental and physical recovery as they interrelate with each other. Think of ways to keep your older loved ones recovering (or in some cases, yourself) motivated. Account for small progress and celebrate them as targets. In addition, speaking to a professional or even confiding in a family member can be beneficial to them getting their thoughts out. While the way life may look may have changed, its new routine does not necessarily have to be viewed through a bad light. Establishing hobbies and a strong support network for senior citizens can prove invaluable during this time.
https://powerfulpatients.org/wp-content/uploads/Seniors.png600600PEN Editorial Staffhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngPEN Editorial Staff2019-06-07 16:17:502024-04-29 12:29:15Helping Seniors With Long Term Recovery: Tips For Carers To Make The Process Easier
https://powerfulpatients.org/wp-content/uploads/FF-Guide-causes.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-05 15:40:502020-10-07 11:42:28Fact or Fiction? AML Causes and Symptoms Program Resource Guide
Dr. Daniel Pollyea, an AML specialist, dispels common myths around the causes and symptoms of AML and shares advice so that you can identify credible resources for information. Download the Program Guide here.
Dr. Daniel A. Pollyea is Clinical Director of Leukemia Services in the Division of Medical Oncology, Hematologic Malignancies and Blood and Marrow Transplant at University of Colorado Cancer Center.
I’m Ross Reynolds. Today we’re gonna be debunking some common misconceptions about the causes and symptoms of AML.
And joining me is Dr. Daniel Pollyea. Dr. Pollyea, could you introduce yourself?
Dr. Pollyea:
Yeah. Hi. Good morning, everyone. I’m Dan Pollyea. I’m an Associate Professor of Medicine here at the University of Colorado, where I am the Clinical Director of Leukemia Service.
Ross:
I wanna emphasize to you that this program is not a substitute for medical advice, so be sure to consult your healthcare team when it comes to solid information about it. But you will get some background that I think you’re gonna find useful. And you might have some questions as we go along.
Dr. Pollyea, let’s start out with the basics. What are the causes of AML?
Dr. Pollyea:
Yeah. So, Acute Myeloid Leukemia, it’s a disease, a cancer of the bone marrow.
And it’s the result of an accumulation of mutation and chromosomal abnormalities that affect the DNA of a precursor cell in the bone marrow, otherwise known as a stem cell.
And those abnormalities accumulate until that cell can no longer properly mature, and it also can’t properly die. And so, a cell like that just makes copy after copy after copy of a cell until it crowds out the whole bone marrow with these sorta useless, immature cells.
And the end result of that is the failure of the bone marrow, which causes all of the problems associated with this disease. So, biologically, that’s sort of what happens to make this disease occur.
Ross:
What are some of the myths that you hear from patients that come in and they say, “Oh, this must’ve caused my AML,” but you have to tell them that’s not so?
Dr. Pollyea:
Right. So, I mean, this is one of the most frustrating issues for patients and their families after diagnosis. I mean, it’s a rare disease, only about 30,000 cases a year in the United States. And so, trying to associate a rare disease with external or environmental factors is difficult to impossible. So, although there are a variety of exposures that probably contribute to this disease, we have very little understanding of what those exposures typically are or how that all works.
So, there’s a few things that we know pretty well; large doses of radiation, either associated with like industrial accidents like the Chernobyl disaster, or some of the radiation therapies that patients receive for other types of cancer. Other types of chemotherapy that are used to cure other cancers can contribute to this disease in later years.
We know that there are certain precursor conditions that can evolve to AML, so a person with myelodysplastic syndrome, for instance, has a fairly high chance of someday evolving to develop Acute Myeloid Leukemia. But beyond these sort of a few associations, there isn’t a whole lot that’s known or proven.
Ross:
Now there is radiation associated with X-rays, and some people think that X-rays can cause AML. Is that true?
Dr. Pollyea:
Yeah.
So, I mean, I think a priori no because millions of people get X-rays every day, and only 30,000 people a year get AML. So, clearly it’s not a simple association between getting an X-ray and developing AML. But I think that there is an unknown interaction between environmental exposures and a person’s individual genetic makeup that makes a person more or less susceptible to developing something like AML with respect to exposure to the environment or X-rays and things.
So, while you cannot say that getting an X-ray will lead to AML, certainly there are some people who are more sensitive to the damage that’s done by something like an X-ray. And so, the best course of action is to be cautious and judicious about your exposure to these things, but not to not get these things when they are medically necessary.
So, that’s the challenging balance.
Ross:
Here’s something else we’ve heard, that weed killers can be a risk factor for AML. Is that true?
Dr. Pollyea:
I mean, I think there’s a lot coming out now about weed killers and their association with other types of cancers. Again, I go back to the limitation we have in that in only 30,000 people a year in the United States get AML. Millions of people are exposed to weed killers.
We’re statistically never going to be able to make a clear association. I think that there are certainly some risks for some people. Whether you’re that person who’s more susceptible to developing leukemia or any other cancer because of exposure to a weed killer is impossible to know.
So, like all of these things, I think the advice we have is you have to live your life. You have to do your best to sort of avoid things that you can avoid that you think would be… Or that may cause problems. But not to let those things prevent you from living a normal life.
I know that’s not a satisfying answer, but at the moment that’s the best answer we have.
Ross:
Is formaldehyde exposure another risk factor for AML?
Dr. Pollyea:
Yeah. We think that it is, and kind of along the lines of benzene. But, again, we think that those studies that have shown those types of association show it in very high amounts, amounts that most people in this country would not be exposed to. But I do think, or we do think that there is something to that, to formaldehyde somehow contributing to this.
Ross:
What’s the difference between a risk factor for AML and a cause of AML?
Dr. Pollyea:
Yeah. So, I think risk factors by definition are things that may contribute to AML. And a risk factor for AML by that definition could be walking down the street and having some exposure to radiation from the sun. A cause of AML is something that is a much more solid sort of well-understood factor.
Like I said before, having myelodysplastic syndrome, there is a high chance that that can evolve to Acute Myeloid Leukemia. And if that happens then the MDS, the myelodysplastic syndrome, could be considered or would be considered the cause of your AML. So, very, very different in terms of the amount of evidence that goes into making those determinations
Ross:
Is there a genetic component to this? Can this run in a family?
Dr. Pollyea:
Yeah. So, this is a disease of the genome.
So, I mean, in a lot of respects it is a genetic disease. But the question is very different when you ask is this an inherited genetic disease? Is this disease due to a gene that I inherited from a parent or could pass along to a child?
For many, many years, the answer from the medical community was, “No.” This was not considered to be a disease that clustered in families or that could be inherited. We now know that that’s not necessarily the case. There are some very rare cases where this does seem to travel in families or cluster in families. And we’re now beginning to understand who those people are and what those genes are.
But the vast majority of people with this disease did not inherit a gene to contribute to it and cannot pass this along to a child. This is a random, spontaneous event that occurred within one person’s own body and is not traveling within family. So, we’re learning more and more about this, but really, the vast majority of this is not an inherited genetic condition.
Ross:
You’ve mentioned gene mutations. What mutates a gene? What causes that to happen that could lead down the line to AML?
Dr. Pollyea:
Yeah. Yeah. That’s a great question. Most of the time we do not know the answer to that. These gene mutations occur spontaneously, randomly, and we don’t understand why they happen when they do happen.
And I know that’s, again, not a satisfying answer. It’s very frustrating, particularly patients come in, and, “I’ve lived a healthy lifestyle. I’ve done everything right. I exercise. I eat right. How could this have happened?”
These are things that for the most part are out of the control of a person. These aren’t impacted by your diet or your activity levels, what you eat or don’t eat, what you do or don’t do. That’s a real frustration. In the end, in almost all cases we don’t know or understand why these gene mutations or these, I call them mistakes in the body, occur when they occur. We don’t understand them.
And, Dr. Pollyea, someone asked if benzene can be a risk factor for AML.
Dr. Pollyea:
Yeah. So, benzene is one of the sort of rare environmental exposure associations that we do have clear associations with AML.
But the level of benzene that a person would need to be exposed to is really something that hasn’t been seen in this country in a very long time.
We’d be talking about like an industrial accident type exposure in almost all cases, so being exposed to a cleaning solution or some other fairly minor exposure to benzene, we don’t think is enough, in most cases, to prompt this disease. But benzene in very high doses, like an industrial accident, yes, that is something that we understand can certainly contribute or cause AML.
Ross:
Autoimmune diseases, such as arthritis, can they increase the risk of AML?
Dr. Pollyea:
Oh, boy. That is a really interesting one. So, there are papers in the literature that do support those associations. And I know in my own practice I certainly see that trend. So, I do think that there is something there. There is a proven association between autoimmune conditions and myelodysplastic syndrome, which I said before can be a clear precursor condition to AML. So, certainly, that is an association that is a possibility.
It can be a little difficult to tease out whether it’s those diseases that are associated with ultimately developing AML, or the treatments that people get for some of those autoimmune diseases. Those treatments can modulate the immune system in certain ways that may, in fact, contribute or drive the disease. So, that’s a difficult thing to tease out.
But in general terms, yes, I think there are some associations. Now not by a long shot everyone with an autoimmune disease gets AML. It’s a teeny, tiny fraction. But I think there is an association there.
Ross:
How easy is it to diagnose AML?
Dr. Pollyea:
Well, I mean, I think there’s very clear diagnostic criteria for AML. But I guess that doesn’t really answer the question. And we certainly have patients who come to us after many months of frustration without a clear diagnosis.
So, those scenarios can play out. Many times AML’s a very dramatic presentation, so people get very, very sick very, very quickly with extraordinarily high white blood cell counts and suppression of all the other blood counts that come from the bone marrow like red blood cells and platelets.
In those cases it’s pretty clear that there is a type of acute leukemia going on. There can be some difficulty distinguishing Acute Myeloid from Acute Lymphoblastic Leukemia; those are sort of like cousins, but very different and treated differently. So, it kinda runs the gamut. I mean, it can be pretty clear, but it’s sometimes missed, so yeah.
Ross:
This is a great lead-in to my next question, which is about the symptoms of AML. What should be the warning signs that this might be something you need to get looked at?
Dr. Pollyea:
Right. So, at presentation, the main symptoms are reflective of the fact that the bone marrow, the organ that makes all the cells of the blood, has failed.
So, that can cause severe anemia. Signs of anemia: a white sort of appearance, feeling dizzy or lightheaded when standing, short of breath, weak, tired, fatigue. Those are all pretty clear presenting symptoms for AML. Because the bone marrow also is responsible for making platelets that clot the blood, some people will present with a bleeding complication, or a very subtle rash made up of these particular red dots. We call that a petechial rash. And that rash can come on when the platelet count gets very low.
Sometimes a person will present with an infection or infections that don’t go away or don’t clear because of decrease in white blood cells, the infection-fighting cells of the bone marrow. Those are made in the bone marrow and can fail in the setting of this disease. So, those are the most common symptoms at presentation, symptoms that are reflective of bone marrow failure.
Ross:
You mentioned that sometimes the presentation could be very dramatic, and it sounds like the symptoms are very severe, very quickly. Is that always the case? Is that often the case?
Dr. Pollyea:
That is the case in, I would say, a minority of times. That’s usually the case. It’s more often seen in younger patients with AML. Typically, older patients with AML have a more smoldering course and a much less dramatic presentation, although this sort of very dramatic and dangerous presentation can happen in older patients, but it’s probably something like a third of the time that those very dramatic and medical emergency presentations occur.
Ross:
How important is early diagnosis?
Dr. Pollyea:
Well, I mean, it’s crucial. I mean, in particular in those cases where it’s a very dramatic and proliferative diagnosis, or presentation. A quick diagnosis and recognition of this condition is very important because the sooner a person starts effective treatment the better the ultimate outcome is.
I would say in general terms that applies to all AML patients, but certainly there’s some degrees of variation. So, there’s some AML patients that when I hear about their case on the phone from a referring doctor, it’s appropriate to see them next week in the clinic.
So, it’s not always a medical emergency, but we would never, even in those next-week-in-the-clinic patients, this isn’t something that can wait for weeks or certainly months. This is something that needs to be addressed fairly quickly.
Ross:
What are the best ways to manage those symptoms?
Dr. Pollyea:
Right. So, I mean, at presentation, all those symptoms, the best way to manage those are to start treatment as quickly as possible. So, impacting the underlying cause of this disease is the most important and critical factor to getting a person feeling better because all of these problems stem from the disease in the bone marrow, and so everything else that you do to sort of help a person’s symptoms are Band-Aids when you’re not talking about getting to the root cause.
So, that’s at presentation. Now once we start treatment, there are many potential side effects to any number of treatments. And it all is dependent on what treatment you’re getting and other things about you that will make this a significant problem in some cases. And in that setting, we do have ways that we can aggressively manage a person’s side effects.
Ross:
Can you manage all of the symptoms? Or can people still be experiencing symptoms even after they’re in treatment?
Dr. Pollyea:
Absolutely. So, a person with this disease, depending on how long they’ve had it and some of the features, may not be feeling back to their baseline self for potentially weeks or months after treatment starts in the best-case scenario. So, that can be very frustrating, but a person needs to sort of be able to continue to have a good outlook and stay positive.
Because we are able in many cases to make a big impact on this disease and return a person to their pre-disease quality of life.
Ross:
What are some of the myths that you hear, Dr. Pollyea, about the treatment? Some things that people come in to you saying they think that it helps, but there’s no science to back that up?
Dr. Pollyea:
So, myths about treatment, so many people have a lot of preconceived notions about the intensity of a therapy that they’re going to be asked to withstand. And although sometimes we do treat this disease very intensively, that’s not always the case, and now we have some very effective lower-intensity regimens that can be used in a variety of different scenarios.
There are a lot of people who have a lot of preconceived notions about a stem-cell transplant or a bone-marrow transplant and whether or not they would be eligible for this based on maybe what they’ve heard from friends or family, or what they’ve seen in the internet.
And those are often incorrect. And so, keeping an open mind about treatment options, and discussing those in detail with your doctor are really, really important.
Ross:
You mentioned sometimes it presents in young people, sometimes in older people. What’s sort of typical?
Dr. Pollyea:
This is a disease of predominantly older patients, so the median age of presentation is 68. So, that means that over half of the patients are over 68 years old at diagnosis. So, while this does happen, can happen in younger patients, that’s really an unusual situation. This disease is, like I said, it is predominantly a disease of older patients.
Ross:
There are some patients who I understand think that supplements can deal with the symptoms of AML. Is that accurate?
Dr. Pollyea:
You know, I mean, I think the supplement question is always a challenge. A lot of these supplements, or most of these supplements have never been tested with the rigor of treatments that we’re accustomed to in the medical establishment.
That being said, I won’t deny that some of the supplements can help patients based on what patients’ experiences are and what they tell me. I think what’s really important is just be very open and honest with your doctor about the supplements that you’re taking or want to take to ensure that there are no sort of unanticipated interactions with treatments.
Because I think most doctors are very open to having their patients care for themselves in the ways that they’ve become accustomed to, and they know their bodies very well, and we’re very open to that. But there are sometimes that a drug or a supplement might have a bad interaction with the treatment.
And so, a good example in my practice is antioxidants. So, there’s a lot of literature, a lot of interest in antioxidants as cancer-prevention treatment.
And a lot of that is not well-established, but still I don’t see much harm. But when it comes time to treating a cancer, that’s a very different situation. When we give a patient treatment to try to kill the cancer cells, many times we’re trying to provoke oxidation. That’s part of how these drugs and these treatments work.
So, if you’re taking those treatments, but also at the same time taking antioxidants, there’s the potential you could sort of be cutting your therapy off at the knees, fighting it with one hand behind your back. So, for the period of time when my patients are getting an active treatment, I ask that they don’t take it antioxidant.
And they can resume that in the future in the hopes of preventing another cancer. But the time to prevent with an antioxidant isn’t appropriate when you’re dealing with an active cancer. So, that’s just one example.
Ross:
Fatigue could be a symptom of AML, but there are a lot of causes of fatigue.
How do you differentiate between something that really could be AML and something that isn’t?
Dr. Pollyea:
Yeah. That’s a challenge because I think these are, as I said, older patients. And older patients have a lot of other medical problems. And older people get fatigued, just that’s unfortunately part of the normal aging process. So, we would usually make an assumption that a person’s fatigue and diagnosis is due to the leukemia, the anemia as a result of the leukemia.
But as we successfully treat a patient if they are responding based on their numbers and other objective criteria, but the fatigue is not improving then I think that’s where we would start to look at other contributing factors, and there can be many, so having an open mind at that point is important.
But at the beginning, this is such a monster of a disease, it’s so overwhelming, I think the focus is usually on assumption that the fatigue is due to the disease or to a treatment associated with this disease.
Ross:
This question: is loss of appetite a symptom of AML?
Dr. Pollyea:
Yeah. I definitely see that, hear that, so sometimes people come in and they say that. Sometimes it may not be a loss of appetite, but an extreme weight loss, so a lot of different types of cancer, including AML, can cause that, just basically unintentional weight loss.
A person’s not trying to lose weight. They’re eating what they think is their normal amount and they’re losing tremendous amounts of weight. So, those are both potential presenting symptoms with AML. And loss of appetite, unfortunately, can be associated with some of the treatments for this disease. And taste changes, things not tasting good, can all contribute to that as well, so those are all challenges that our patients face.
Ross:
How important is to get a second opinion? I mean, are all doctors like you pretty much on the same page when it comes to symptoms and treatment?
Dr. Pollyea:
So, this is a challenge. So, the answer to the second question first is unfortunately, no. A lot of this hasn’t quite been standardized. And some doctors, oncologists, cancer doctors, they’ll predominantly be treating the things that are common: colon cancer, breast cancer, prostate cancer. And they will probably only have a few cases of acute leukemia a year.
And so, their approach to this is going to be different than somebody who spends all day seeing patients with AML and thinking about AML.
So, a second opinion is a very nice thing to be able to do. The problem with this disease is that most times it doesn’t afford that opportunity. So, with other conditions you have some time to go out, read about it, talk to some different doctors, get a good plan together.
With AML, often that’s not a possibility. A person is so urgently sick that you have to sorta deal with the resources where you are. The best recommendation I have there, if you do find yourself in a situation where there’s not a lot of expertise is to ask your doctor to just call somebody in the region or email somebody in the region who may have that expertise.
And most doctors all over the country have that sort of resource or partner that they will go to and talk the case through with them, and maybe a transfer to one of those high-volume centers is appropriate.
And maybe that’s not a possibility or appropriate, but maybe you would benefit from just talking… Maybe your doctor would benefit from talking this through. But in cases where it’s not such a dramatic presentation, then yeah, for sure, I think a second opinion can be appropriate. But this isn’t something that can be sort of drawn out for long period of time.
Ross:
You know, when you find out something like this, your tendency might be to jump on the web and start searching for AML. How do you vet those sources that you look at? How do you figure out that their – what would be a sign that they’re bogus sources?
Dr. Pollyea:
Yeah. I mean, I think this field is so rapidly changing and the treatment that we have, that I would, for the most part, assume that what you’re finding on the web is not relevant and is not an up-to-date resource. So, the resources that I listed, the NCCN, UpToDate, the Leukemia & Lymphoma Society, I should mention.
A very important resource that has up-to-date information, and they have even phone numbers for patients and their families to call to get connected with the proper people in a particular city, so that is a really important resource. But I’d be really, really cautious about what you find on the internet because things are changing so fast in this field. There’s a lot of outdated and misinformation on the internet.
Ross:
Well, then there’s outright scams. One of the things you mentioned before we went on is be cautious if someone’s asking you to put money upfront, or if it’s a nonmedical facility. What are some things that people should watch out for?
Dr. Pollyea:
Yeah. So, one of the things that is so important in our area is clinical trials and participating in clinical trials. Patients who opt to do this and receive experimental therapies can sometimes get the treatment of the future, get a drug that’s not currently available through the FDA, but may have a lot of promise.
And this is the way that we fight this disease. We’ve recently had an onslaught of approvals for AML and that’s because the patients being willing to participate in sanctioned clinical trials. So, participating in a sanctioned clinical trial is crucial, and it’s always a recommendation of all leukemia doctors.
When you participate in a conventional clinical trial, you’re asked to sign a consent form that explains what you’re doing and why. There is a confirmation that this has been vetted by an institution’s regulatory board that is prioritizing the safety and well-being of you, the patient. This has been approved by the FDA as a clinical trial. Nobody would ever ask you to pay money. That’s not ethical to participate in a clinical trial. Insurance covers whatever standard of care. And the clinical trial covers anything that isn’t.
So, if you find yourself in a situation where you’re not being asked to sign a consent form, where a clinical trial has not been reviewed by a regulatory board, where your doctor is not a leukemia specialist, where the FDA has not sanctioned the treatment, all of those are alarm signs.
Because there are people out there that are preying on patients in a desperate situation, a very difficult time in their life, and giving them sort of false hope and leading them down paths that are not legitimate.
One easy thing to do to sorta check to see if a clinical trial is legitimate is to go onto clinicaltrials.gov.
This is a resource set up by our national healthcare system that now feeds in every legitimate clinical trial from all over the world, needs to be registered on clinicaltrials.gov. So, if you can’t find your clinical trial on clinicaltrials.gov, I would have a lot skepticism and caution about that.
Ross:
Like what advice do you have for people when they’re first diagnosed? What are the first things they should try to do?
Dr. Pollyea:
Yeah. I mean, that reaction is totally normal and natural. I mean, many times these people are perfectly healthy or have been perfectly healthy, and this news is a complete shock.
And so, it is normal and appropriate to have some period of grieving for the healthy life that you are losing. But I would also, while giving yourself that time to grieve, first, draw on your support system, your family, your friends. Allow them to help you. Accept that assistance that they have. And to be optimistic because we are getting so much better at treating this disease.
I had mentioned before, there has been an onslaught of approvals for drugs in this area the likes of which hasn’t been seen in decades. We have new tools and weapons in our arsenal that we couldn’t have dreamed of even a few years ago.
We in our community are very excited and hopeful about the future and we hope that that will translate ultimately to patients, but being depressed or being down, being scared, all of that is normal.
All of that is expected. Anyone would feel like that. Allowing yourself to have those feelings and emotions is important, as long as it doesn’t get in the way of doing what you need to do to fight this disease.
Ross:
It sounds like you’re hopeful about new treatments for the disease. How about a cure? What’s the science? What’s the medical science say about that? Are we getting any closer to that?
Dr. Pollyea:
We are getting closer to curing this in more cases. So, like I mentioned before, as bad as this is, we can already cure some subsets of patients. There’s one type of Acute Myeloid Leukemia called Acute Promyelocytic Leukemia, APL. It’s an uncommon form of AML, less than 10 percent.
But we can cure close to 99 percent of people with APL. And APL, 15 years ago, was universally the worst form of acute leukemia to get. So, that dramatic 180 that we’ve seen in APL, we are hoping to translate into other forms of AML.
Some other forms of AML have cure rates as high as 50 percent, 60 percent, 70 percent in the right setting. Sometimes we can cure patients with a stem cell transplant fairly reliably. So, we are very, very hopeful about our ability to continue to make progress and cure more and more and more of these patients. That’s the future that we see.
Ross:
Dr. Pollyea, thank you so much. And thank you so much for ending on such a positive note. We really appreciate it. And thank you for joining us for this program today.
To learn more about AML and to access tools to help you become a proactive patient, visit powerfulpatients.org. I’m Ross Reynolds. Thanks for joining us.
https://powerfulpatients.org/wp-content/uploads/Pollyea-1.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-05 15:38:122022-09-08 12:04:58Fact or Fiction? AML Causes & Symptoms
Dogs and humans have shared a special bond for over 12,000 years. Clinical research has shown that dogs increase quality of life, finding that those living alone with a dog have a 33% decreased risk of death. A study published by the Complementary Health Practice Review also found that pet owners are likely to have lower blood pressure, better cognitive function, and decreased anxiety than their non-pet owning counterparts. For those fighting a long term or chronic illness, spending time with a dog can have broad health benefits for both the body and the mind.
Mental Health
A long term hospital stay is difficult for patients, particularly those in critical care units. Even physicians with exceptional bedside manner can only do so much to mitigate the clinical nature of a hospital room. A study published in Critical Care shows that animal therapy can help ICU patients overcome the mental health issues associated with an extended hospital stay. Bringing in a dog to engage with patients breaks up the monotony of the hospital, and improves mood. 74% of pet owners report improvements in mental health, showing that dogs lessen feelings of loneliness and isolation.
Dementia And Alzheimer’s
Patients in nursing homes go through many of the same problems as those battling in an ICU. Nursing homes pose a particularly great challenge for those with dementia and Alzheimers, as unfamiliar settings and faces can cause distress. A promising study published in the American Journal of Alzheimer’s Disease and Other Dementias shows that dementia patients enrolled in animal-assisted therapy had decreased levels of agitation and greater social interaction than a control group. Notably, many of the patients involved in the study had owned dogs in the past. A key part of treating dementia-type disorders is involving patients in activities that they have enjoyed over the course of their life. For animal lovers in nursing homes, playing with a dog for even a few hours a week can have a massive impact on their quality of life.
Exercise And Physical Fitness
Most dogs are seemingly boundless, furry balls of energy – particularly high energy, social breeds such as Black German Shepherds. Walking and playing with a high energy dog is necessary for their happiness, and comes with the obvious benefit of weight loss and a decreased chance of diabetes for people as well. The benefits of playing with a dog can be much broader than weight loss. Exercise is a vital part of physical rehabilitation, and has shown to cause remission of major depressive disorder on par with antidepressants in clinical trials. Coupled with the effort required to keep them healthy, a dog can give a person recovering from an illness a greater sense of purpose, which helps patients mentally as well as physically.
Registering a therapy dog requires a bit of work, but is a worthwhile vocation for both dog and owner. While medications and in-patient care are necessary for many illnesses, a visit from a dog can help make the arduous process of getting healthy a little less taxing and far more rewarding.
https://powerfulpatients.org/wp-content/uploads/Four-Legged-Physician.png600600PEN Editorial Staffhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngPEN Editorial Staff2019-05-06 17:19:132022-11-08 13:58:00Four-Legged Physicians: How Dogs Can Aid Patient Therapy
 Find Your Voice Resource Guide
Find Your Voice Resource Guide Office Visit Planner
Office Visit Planner Why Speaking Up Matter: Tips From an AML Advocate
Why Speaking Up Matter: Tips From an AML Advocate