Your Acute Myeloid Leukemia (AML) diagnosis is just a starting point. Even though the path ahead may seem unclear or even insurmountable, armed with knowledge you can take control.
When people are anxious about their diagnosis, I think the best thing to do is to keep an eye on the bigger picture. I know your life is going to change. We can’t even make plans more than one week ahead of time. So, it’s important to keep an eye on the bigger picture. And the bigger picture is this is a steppingstone in your journey. This is a place, a situation, that you’re placed in that you’re having to undergo. But overall, you have a life outside of AML. You’ve had a life outside of AML. And keeping that bigger picture in the back of your head is very important. It’s very sane. You had a life. You enjoyed things before. You enjoyed going to the movies. You enjoy having dinners with your friends. You enjoy reading books. And so, it’s very healthy to continue to do those things and not get so consumed by the AML diagnosis and what is going on.
It will affect your life and it’s very important to keep doing what you’re doing. If you exercise, continue exercising. If you enjoy going to the movies, continue going to the movies with the expectation that you may not do that all of the time as you did before but you, certainly, can continue to do that because it keeps your head clear. It keeps you human because so much of AML takes away from you and you feel like you’re this thing, you’re this number. You’re the medical record number. You are Mr. so and so or you are a diagnosis. You are an AML diagnosis. It keeps you human to keep an eye on the bigger picture.
https://powerfulpatients.org/wp-content/uploads/Overcoming-Anxiety.png600600Caitlin McDonaldhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngCaitlin McDonald2019-06-27 18:57:412022-10-25 13:16:17Overcoming the Anxiety of an AML Diagnosis
Mayra Lee, a Registered Nurse, explains the positive benefits of educating yourself about AML and outlines key steps for learning more about your disease. Download the Find Your Voice Resource Guide here.
Mayra Lee, RN, is an outpatient clinic nurse at Moffitt Cancer Center. More about the expert.
So, the benefit of becoming informed about your disease when you’re diagnosed with AML would be that you are empowered. You will be empowered to – so much control is lost when you hear the word cancer. So much of your life changes in a matter of days or weeks from the time you’re told you have AML. Becoming informed about the treatments, about your disease, about what it is, about what the next step is empowers you to have control of the disease again when so much of your life is going to be out of control. It makes you be the driver in the disease along with your medical team. The medical team will steer you in which direction we think we should go but you will, ultimately, be the one making the decision with your team. You will not feel like the decision was made by your doctor. The decision is made together as it should be. The patient, the family, and the physicians and the team of medical people that take care of you.
It will not be something that your doctor does alone or that you’re doing alone because this is a very long journey, a very tedious journey. And the more you know about it also the less scared and the less stressed out you are about the diagnosis itself.
Patients can take key steps such as to become informed about their disease such as I think the first step would be to pick up those informational books or educational books that you will see out in the lobby in most physicians’ offices about AML, what is AML. That is step No. 1. Asking the nurses and the doctors do you have any information on my diagnosis, is there a reputable website that you recommend. There is a lot out there on the internet but a lot is not reputable and a lot is just hearsay.
And a lot of it is patients sharing in their own stories, which are all good formats but in the very beginning, you want to go to reputable websites. You want to hear it from NCCN or any one of those websites that have really good information about what the disease really is. And then, you can navigate whichever way you want, if you want to join those forums. And then, you’re better informed and you’re better educated as to what to expect.
https://powerfulpatients.org/wp-content/uploads/AML-Educated.png600600Caitlin McDonaldhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngCaitlin McDonald2019-06-21 18:54:552022-10-25 13:16:17Why Should You Become Educated about Your AML?
Registered nurse, Mayra Lee, outlines essential steps for making the most of appointments with your AML team. Download the Office Visit Planner and bring it to your next appointment here.
Mayra Lee, RN, is an outpatient clinic nurse at Moffitt Cancer Center. More about the expert.
During an initial visit, patients often forget to ask about how the treatment for their AML cancer is going to impact the quality of their life and all of the things that they do on a daily basis and being impacted by such a treatment. Treatments are, often times, discussed about we’re going to do X chemo or Y chemo, seven plus three, three plus seven, five days on Dacogen, whatever it may be. But the patients don’t often grasp the amount of quality of life that will be taken from their lives.
Other things that impact the quality of their life is a financial burden that the treatments bring about, having caretakers around them. We often see patients that don’t have a lot of family members or don’t have family here in the state that they’re residing in and they don’t have a lot of support. So, these are all things that are going to be impacted by the treatments for AML. And a lot of times, patients don’t ask that question very clearly about what is the realistic expectations of my life during the treatment phase.
Patients can best prepare for an office visit by asking questions, writing down the questions, before they come to the office and having it prepared.
And I think it’s very important for patients to write those questions down before they come to their treatment. It’s also very important to bring a note pad and a pen and write down things that are being said during your visit, whether it be the first time you hear this or a second or third opinion is very important to write down treatments. It’s important to write down things that you might not have picked up on the first visit when you were first diagnosed like chromosomes and different treatments and different tests that are going to be ordered. It’ very difficult to retain all of that information in one sitting. So, it’s important to bring a note pad and bring a friend to write those things down with you.
It’s very important to bring a family member or a friend to your appointments because that person – you can bounce back ideas and you can bounce back information.
You’re not there alone and it makes you feel like you’re not carrying the burden of now distributing this information to your friends and your family who are, obviously, very worried about you, your prognosis, your diagnosis, what did the doctor say. And you have someone else to say oh, they said this or the doctor said that. And you will not remember everything that was said in one sitting. So, bringing your friend or family member helps put all of that information together and helps recall everything that was said in that visit.
https://powerfulpatients.org/wp-content/uploads/AML-Team.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-17 19:08:432022-11-08 14:22:56Optimize Your First Visit with Your AML Team
Dr. Elizabeth Bowhay-Carnes provides advice for patients facing an AML diagnosis, including the necessity of putting together a strong healthcare team and leaning on your personal support system. Download the Find Your Voice Resource Guide here.
Dr. Elizabeth Bowhay–Carnes is Director of the Adult Non-Malignant Hematology Program and Co-Director of the Adolescent/Young Adult Oncology Program at Mays Cancer Center, home to UT Health San Antonio MD Anderson Cancer Center. More about this expert.
My name is Dr. Elizabeth Bowhay-Carnes. I work at UT Health San Antonio MD Anderson Cancer Center, and I am a blood specialist. I specialize in taking care of patients that have various blood disorders, and my passion is working with patients and their families when someone is diagnosed with a blood cancer.
If I was a patient who was diagnosed with AML today, the first thing I would want to do is take a deep breath. When somebody is diagnosed with AML, this is a disorder that comes on suddenly, and so usually a patient and family are in shock. Usually, somebody was perfectly healthy a couple weeks before their presentation and then they find themselves admitted in a hospital, or a hospital setting, feeling quite ill. And so, one of the first things I would do is to make sure I understand who my care team will be. Fighting cancer is a team sport.
It is not an individual event. Although the patient is the most valuable player, there’s different parts of the team that are needed to get somebody through this diagnosis and their treatment. If I was the patient, I would make sure I understood who would be in charge of my treatment plan or who would be the attending physician. I would want to know who the main nursing contact or support person would be. If there’s calls in the middle of the night or emergencies, who’s the first person to call? I would want to make sure I have a family or friend support person designated as the main supportive role, who would help me fight through this process. Again, if I was diagnosed with AML today, I would take a deep breath, and I would re-center myself and establish who my care team would be.
https://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.png00Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-12 16:44:122022-10-25 13:16:16What Would You Do? AML Advice From An Expert
Brittany DeGreef, a genetic counselor, provides essential advice for when you are facing a cancer diagnosis emphasizing that leaning on supportive friends and family is key. Download the Office Visit Planner and bring it to your next appointment here.
Brittany Degreef is a Genetic Counselor at Robert H. Lurie Comprehensive Cancer Center of Northwestern University. More about this expert.
One piece of advice I give patients who are just diagnosed with cancer – and we do frequently see patients at least once a week who were just diagnosed either that week or the week prior – is feel what you need to feel. Not every patient is going to react or cope with their diagnosis in the same way as someone next to them, even within the same family. That also goes for caregivers and relatives.
So, just because you feel like helping out a relative in a specific way, it might not be the same for your brother or sister or cousin.
So, we always tell patients that there is no wrong or right way to cope with a diagnosis of cancer. The way that you approach it is perfectly fine and there’s no right or wrong way to do that.
So, another piece of advice we always tell patients is don’t be scared to lean on your support network, whether that be family or friends, your healthcare provider, advocacy groups, never be afraid to ask for help.
And for some patients who feel like they have limited resources, usually hospitals where you’re receiving your patient care has many resources available to you, whether that be emotional, financial, spiritual, logistical. Don’t be scared to ask about those resources.
https://powerfulpatients.org/wp-content/uploads/advice.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-12 16:22:532022-10-25 13:16:16Facing a Cancer Diagnosis: Advice From An Expert
Appointments with your physician can be overwhelming. To optimize your visit, it’s best to arrive organized and prepared to take notes. Our Office Visit Planner can help. Guides for your first office visit as well as your follow-up office visit, tailored for patients and caregivers, are available below. Download, print and bring along with you to the appointment.
https://powerfulpatients.org/wp-content/uploads/FF-Guide-causes.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-05 15:40:502020-10-07 11:42:28Fact or Fiction? AML Causes and Symptoms Program Resource Guide
Dr. Daniel Pollyea, an AML specialist, dispels common myths around the causes and symptoms of AML and shares advice so that you can identify credible resources for information. Download the Program Guide here.
Dr. Daniel A. Pollyea is Clinical Director of Leukemia Services in the Division of Medical Oncology, Hematologic Malignancies and Blood and Marrow Transplant at University of Colorado Cancer Center.
I’m Ross Reynolds. Today we’re gonna be debunking some common misconceptions about the causes and symptoms of AML.
And joining me is Dr. Daniel Pollyea. Dr. Pollyea, could you introduce yourself?
Dr. Pollyea:
Yeah. Hi. Good morning, everyone. I’m Dan Pollyea. I’m an Associate Professor of Medicine here at the University of Colorado, where I am the Clinical Director of Leukemia Service.
Ross:
I wanna emphasize to you that this program is not a substitute for medical advice, so be sure to consult your healthcare team when it comes to solid information about it. But you will get some background that I think you’re gonna find useful. And you might have some questions as we go along.
Dr. Pollyea, let’s start out with the basics. What are the causes of AML?
Dr. Pollyea:
Yeah. So, Acute Myeloid Leukemia, it’s a disease, a cancer of the bone marrow.
And it’s the result of an accumulation of mutation and chromosomal abnormalities that affect the DNA of a precursor cell in the bone marrow, otherwise known as a stem cell.
And those abnormalities accumulate until that cell can no longer properly mature, and it also can’t properly die. And so, a cell like that just makes copy after copy after copy of a cell until it crowds out the whole bone marrow with these sorta useless, immature cells.
And the end result of that is the failure of the bone marrow, which causes all of the problems associated with this disease. So, biologically, that’s sort of what happens to make this disease occur.
Ross:
What are some of the myths that you hear from patients that come in and they say, “Oh, this must’ve caused my AML,” but you have to tell them that’s not so?
Dr. Pollyea:
Right. So, I mean, this is one of the most frustrating issues for patients and their families after diagnosis. I mean, it’s a rare disease, only about 30,000 cases a year in the United States. And so, trying to associate a rare disease with external or environmental factors is difficult to impossible. So, although there are a variety of exposures that probably contribute to this disease, we have very little understanding of what those exposures typically are or how that all works.
So, there’s a few things that we know pretty well; large doses of radiation, either associated with like industrial accidents like the Chernobyl disaster, or some of the radiation therapies that patients receive for other types of cancer. Other types of chemotherapy that are used to cure other cancers can contribute to this disease in later years.
We know that there are certain precursor conditions that can evolve to AML, so a person with myelodysplastic syndrome, for instance, has a fairly high chance of someday evolving to develop Acute Myeloid Leukemia. But beyond these sort of a few associations, there isn’t a whole lot that’s known or proven.
Ross:
Now there is radiation associated with X-rays, and some people think that X-rays can cause AML. Is that true?
Dr. Pollyea:
Yeah.
So, I mean, I think a priori no because millions of people get X-rays every day, and only 30,000 people a year get AML. So, clearly it’s not a simple association between getting an X-ray and developing AML. But I think that there is an unknown interaction between environmental exposures and a person’s individual genetic makeup that makes a person more or less susceptible to developing something like AML with respect to exposure to the environment or X-rays and things.
So, while you cannot say that getting an X-ray will lead to AML, certainly there are some people who are more sensitive to the damage that’s done by something like an X-ray. And so, the best course of action is to be cautious and judicious about your exposure to these things, but not to not get these things when they are medically necessary.
So, that’s the challenging balance.
Ross:
Here’s something else we’ve heard, that weed killers can be a risk factor for AML. Is that true?
Dr. Pollyea:
I mean, I think there’s a lot coming out now about weed killers and their association with other types of cancers. Again, I go back to the limitation we have in that in only 30,000 people a year in the United States get AML. Millions of people are exposed to weed killers.
We’re statistically never going to be able to make a clear association. I think that there are certainly some risks for some people. Whether you’re that person who’s more susceptible to developing leukemia or any other cancer because of exposure to a weed killer is impossible to know.
So, like all of these things, I think the advice we have is you have to live your life. You have to do your best to sort of avoid things that you can avoid that you think would be… Or that may cause problems. But not to let those things prevent you from living a normal life.
I know that’s not a satisfying answer, but at the moment that’s the best answer we have.
Ross:
Is formaldehyde exposure another risk factor for AML?
Dr. Pollyea:
Yeah. We think that it is, and kind of along the lines of benzene. But, again, we think that those studies that have shown those types of association show it in very high amounts, amounts that most people in this country would not be exposed to. But I do think, or we do think that there is something to that, to formaldehyde somehow contributing to this.
Ross:
What’s the difference between a risk factor for AML and a cause of AML?
Dr. Pollyea:
Yeah. So, I think risk factors by definition are things that may contribute to AML. And a risk factor for AML by that definition could be walking down the street and having some exposure to radiation from the sun. A cause of AML is something that is a much more solid sort of well-understood factor.
Like I said before, having myelodysplastic syndrome, there is a high chance that that can evolve to Acute Myeloid Leukemia. And if that happens then the MDS, the myelodysplastic syndrome, could be considered or would be considered the cause of your AML. So, very, very different in terms of the amount of evidence that goes into making those determinations
Ross:
Is there a genetic component to this? Can this run in a family?
Dr. Pollyea:
Yeah. So, this is a disease of the genome.
So, I mean, in a lot of respects it is a genetic disease. But the question is very different when you ask is this an inherited genetic disease? Is this disease due to a gene that I inherited from a parent or could pass along to a child?
For many, many years, the answer from the medical community was, “No.” This was not considered to be a disease that clustered in families or that could be inherited. We now know that that’s not necessarily the case. There are some very rare cases where this does seem to travel in families or cluster in families. And we’re now beginning to understand who those people are and what those genes are.
But the vast majority of people with this disease did not inherit a gene to contribute to it and cannot pass this along to a child. This is a random, spontaneous event that occurred within one person’s own body and is not traveling within family. So, we’re learning more and more about this, but really, the vast majority of this is not an inherited genetic condition.
Ross:
You’ve mentioned gene mutations. What mutates a gene? What causes that to happen that could lead down the line to AML?
Dr. Pollyea:
Yeah. Yeah. That’s a great question. Most of the time we do not know the answer to that. These gene mutations occur spontaneously, randomly, and we don’t understand why they happen when they do happen.
And I know that’s, again, not a satisfying answer. It’s very frustrating, particularly patients come in, and, “I’ve lived a healthy lifestyle. I’ve done everything right. I exercise. I eat right. How could this have happened?”
These are things that for the most part are out of the control of a person. These aren’t impacted by your diet or your activity levels, what you eat or don’t eat, what you do or don’t do. That’s a real frustration. In the end, in almost all cases we don’t know or understand why these gene mutations or these, I call them mistakes in the body, occur when they occur. We don’t understand them.
And, Dr. Pollyea, someone asked if benzene can be a risk factor for AML.
Dr. Pollyea:
Yeah. So, benzene is one of the sort of rare environmental exposure associations that we do have clear associations with AML.
But the level of benzene that a person would need to be exposed to is really something that hasn’t been seen in this country in a very long time.
We’d be talking about like an industrial accident type exposure in almost all cases, so being exposed to a cleaning solution or some other fairly minor exposure to benzene, we don’t think is enough, in most cases, to prompt this disease. But benzene in very high doses, like an industrial accident, yes, that is something that we understand can certainly contribute or cause AML.
Ross:
Autoimmune diseases, such as arthritis, can they increase the risk of AML?
Dr. Pollyea:
Oh, boy. That is a really interesting one. So, there are papers in the literature that do support those associations. And I know in my own practice I certainly see that trend. So, I do think that there is something there. There is a proven association between autoimmune conditions and myelodysplastic syndrome, which I said before can be a clear precursor condition to AML. So, certainly, that is an association that is a possibility.
It can be a little difficult to tease out whether it’s those diseases that are associated with ultimately developing AML, or the treatments that people get for some of those autoimmune diseases. Those treatments can modulate the immune system in certain ways that may, in fact, contribute or drive the disease. So, that’s a difficult thing to tease out.
But in general terms, yes, I think there are some associations. Now not by a long shot everyone with an autoimmune disease gets AML. It’s a teeny, tiny fraction. But I think there is an association there.
Ross:
How easy is it to diagnose AML?
Dr. Pollyea:
Well, I mean, I think there’s very clear diagnostic criteria for AML. But I guess that doesn’t really answer the question. And we certainly have patients who come to us after many months of frustration without a clear diagnosis.
So, those scenarios can play out. Many times AML’s a very dramatic presentation, so people get very, very sick very, very quickly with extraordinarily high white blood cell counts and suppression of all the other blood counts that come from the bone marrow like red blood cells and platelets.
In those cases it’s pretty clear that there is a type of acute leukemia going on. There can be some difficulty distinguishing Acute Myeloid from Acute Lymphoblastic Leukemia; those are sort of like cousins, but very different and treated differently. So, it kinda runs the gamut. I mean, it can be pretty clear, but it’s sometimes missed, so yeah.
Ross:
This is a great lead-in to my next question, which is about the symptoms of AML. What should be the warning signs that this might be something you need to get looked at?
Dr. Pollyea:
Right. So, at presentation, the main symptoms are reflective of the fact that the bone marrow, the organ that makes all the cells of the blood, has failed.
So, that can cause severe anemia. Signs of anemia: a white sort of appearance, feeling dizzy or lightheaded when standing, short of breath, weak, tired, fatigue. Those are all pretty clear presenting symptoms for AML. Because the bone marrow also is responsible for making platelets that clot the blood, some people will present with a bleeding complication, or a very subtle rash made up of these particular red dots. We call that a petechial rash. And that rash can come on when the platelet count gets very low.
Sometimes a person will present with an infection or infections that don’t go away or don’t clear because of decrease in white blood cells, the infection-fighting cells of the bone marrow. Those are made in the bone marrow and can fail in the setting of this disease. So, those are the most common symptoms at presentation, symptoms that are reflective of bone marrow failure.
Ross:
You mentioned that sometimes the presentation could be very dramatic, and it sounds like the symptoms are very severe, very quickly. Is that always the case? Is that often the case?
Dr. Pollyea:
That is the case in, I would say, a minority of times. That’s usually the case. It’s more often seen in younger patients with AML. Typically, older patients with AML have a more smoldering course and a much less dramatic presentation, although this sort of very dramatic and dangerous presentation can happen in older patients, but it’s probably something like a third of the time that those very dramatic and medical emergency presentations occur.
Ross:
How important is early diagnosis?
Dr. Pollyea:
Well, I mean, it’s crucial. I mean, in particular in those cases where it’s a very dramatic and proliferative diagnosis, or presentation. A quick diagnosis and recognition of this condition is very important because the sooner a person starts effective treatment the better the ultimate outcome is.
I would say in general terms that applies to all AML patients, but certainly there’s some degrees of variation. So, there’s some AML patients that when I hear about their case on the phone from a referring doctor, it’s appropriate to see them next week in the clinic.
So, it’s not always a medical emergency, but we would never, even in those next-week-in-the-clinic patients, this isn’t something that can wait for weeks or certainly months. This is something that needs to be addressed fairly quickly.
Ross:
What are the best ways to manage those symptoms?
Dr. Pollyea:
Right. So, I mean, at presentation, all those symptoms, the best way to manage those are to start treatment as quickly as possible. So, impacting the underlying cause of this disease is the most important and critical factor to getting a person feeling better because all of these problems stem from the disease in the bone marrow, and so everything else that you do to sort of help a person’s symptoms are Band-Aids when you’re not talking about getting to the root cause.
So, that’s at presentation. Now once we start treatment, there are many potential side effects to any number of treatments. And it all is dependent on what treatment you’re getting and other things about you that will make this a significant problem in some cases. And in that setting, we do have ways that we can aggressively manage a person’s side effects.
Ross:
Can you manage all of the symptoms? Or can people still be experiencing symptoms even after they’re in treatment?
Dr. Pollyea:
Absolutely. So, a person with this disease, depending on how long they’ve had it and some of the features, may not be feeling back to their baseline self for potentially weeks or months after treatment starts in the best-case scenario. So, that can be very frustrating, but a person needs to sort of be able to continue to have a good outlook and stay positive.
Because we are able in many cases to make a big impact on this disease and return a person to their pre-disease quality of life.
Ross:
What are some of the myths that you hear, Dr. Pollyea, about the treatment? Some things that people come in to you saying they think that it helps, but there’s no science to back that up?
Dr. Pollyea:
So, myths about treatment, so many people have a lot of preconceived notions about the intensity of a therapy that they’re going to be asked to withstand. And although sometimes we do treat this disease very intensively, that’s not always the case, and now we have some very effective lower-intensity regimens that can be used in a variety of different scenarios.
There are a lot of people who have a lot of preconceived notions about a stem-cell transplant or a bone-marrow transplant and whether or not they would be eligible for this based on maybe what they’ve heard from friends or family, or what they’ve seen in the internet.
And those are often incorrect. And so, keeping an open mind about treatment options, and discussing those in detail with your doctor are really, really important.
Ross:
You mentioned sometimes it presents in young people, sometimes in older people. What’s sort of typical?
Dr. Pollyea:
This is a disease of predominantly older patients, so the median age of presentation is 68. So, that means that over half of the patients are over 68 years old at diagnosis. So, while this does happen, can happen in younger patients, that’s really an unusual situation. This disease is, like I said, it is predominantly a disease of older patients.
Ross:
There are some patients who I understand think that supplements can deal with the symptoms of AML. Is that accurate?
Dr. Pollyea:
You know, I mean, I think the supplement question is always a challenge. A lot of these supplements, or most of these supplements have never been tested with the rigor of treatments that we’re accustomed to in the medical establishment.
That being said, I won’t deny that some of the supplements can help patients based on what patients’ experiences are and what they tell me. I think what’s really important is just be very open and honest with your doctor about the supplements that you’re taking or want to take to ensure that there are no sort of unanticipated interactions with treatments.
Because I think most doctors are very open to having their patients care for themselves in the ways that they’ve become accustomed to, and they know their bodies very well, and we’re very open to that. But there are sometimes that a drug or a supplement might have a bad interaction with the treatment.
And so, a good example in my practice is antioxidants. So, there’s a lot of literature, a lot of interest in antioxidants as cancer-prevention treatment.
And a lot of that is not well-established, but still I don’t see much harm. But when it comes time to treating a cancer, that’s a very different situation. When we give a patient treatment to try to kill the cancer cells, many times we’re trying to provoke oxidation. That’s part of how these drugs and these treatments work.
So, if you’re taking those treatments, but also at the same time taking antioxidants, there’s the potential you could sort of be cutting your therapy off at the knees, fighting it with one hand behind your back. So, for the period of time when my patients are getting an active treatment, I ask that they don’t take it antioxidant.
And they can resume that in the future in the hopes of preventing another cancer. But the time to prevent with an antioxidant isn’t appropriate when you’re dealing with an active cancer. So, that’s just one example.
Ross:
Fatigue could be a symptom of AML, but there are a lot of causes of fatigue.
How do you differentiate between something that really could be AML and something that isn’t?
Dr. Pollyea:
Yeah. That’s a challenge because I think these are, as I said, older patients. And older patients have a lot of other medical problems. And older people get fatigued, just that’s unfortunately part of the normal aging process. So, we would usually make an assumption that a person’s fatigue and diagnosis is due to the leukemia, the anemia as a result of the leukemia.
But as we successfully treat a patient if they are responding based on their numbers and other objective criteria, but the fatigue is not improving then I think that’s where we would start to look at other contributing factors, and there can be many, so having an open mind at that point is important.
But at the beginning, this is such a monster of a disease, it’s so overwhelming, I think the focus is usually on assumption that the fatigue is due to the disease or to a treatment associated with this disease.
Ross:
This question: is loss of appetite a symptom of AML?
Dr. Pollyea:
Yeah. I definitely see that, hear that, so sometimes people come in and they say that. Sometimes it may not be a loss of appetite, but an extreme weight loss, so a lot of different types of cancer, including AML, can cause that, just basically unintentional weight loss.
A person’s not trying to lose weight. They’re eating what they think is their normal amount and they’re losing tremendous amounts of weight. So, those are both potential presenting symptoms with AML. And loss of appetite, unfortunately, can be associated with some of the treatments for this disease. And taste changes, things not tasting good, can all contribute to that as well, so those are all challenges that our patients face.
Ross:
How important is to get a second opinion? I mean, are all doctors like you pretty much on the same page when it comes to symptoms and treatment?
Dr. Pollyea:
So, this is a challenge. So, the answer to the second question first is unfortunately, no. A lot of this hasn’t quite been standardized. And some doctors, oncologists, cancer doctors, they’ll predominantly be treating the things that are common: colon cancer, breast cancer, prostate cancer. And they will probably only have a few cases of acute leukemia a year.
And so, their approach to this is going to be different than somebody who spends all day seeing patients with AML and thinking about AML.
So, a second opinion is a very nice thing to be able to do. The problem with this disease is that most times it doesn’t afford that opportunity. So, with other conditions you have some time to go out, read about it, talk to some different doctors, get a good plan together.
With AML, often that’s not a possibility. A person is so urgently sick that you have to sorta deal with the resources where you are. The best recommendation I have there, if you do find yourself in a situation where there’s not a lot of expertise is to ask your doctor to just call somebody in the region or email somebody in the region who may have that expertise.
And most doctors all over the country have that sort of resource or partner that they will go to and talk the case through with them, and maybe a transfer to one of those high-volume centers is appropriate.
And maybe that’s not a possibility or appropriate, but maybe you would benefit from just talking… Maybe your doctor would benefit from talking this through. But in cases where it’s not such a dramatic presentation, then yeah, for sure, I think a second opinion can be appropriate. But this isn’t something that can be sort of drawn out for long period of time.
Ross:
You know, when you find out something like this, your tendency might be to jump on the web and start searching for AML. How do you vet those sources that you look at? How do you figure out that their – what would be a sign that they’re bogus sources?
Dr. Pollyea:
Yeah. I mean, I think this field is so rapidly changing and the treatment that we have, that I would, for the most part, assume that what you’re finding on the web is not relevant and is not an up-to-date resource. So, the resources that I listed, the NCCN, UpToDate, the Leukemia & Lymphoma Society, I should mention.
A very important resource that has up-to-date information, and they have even phone numbers for patients and their families to call to get connected with the proper people in a particular city, so that is a really important resource. But I’d be really, really cautious about what you find on the internet because things are changing so fast in this field. There’s a lot of outdated and misinformation on the internet.
Ross:
Well, then there’s outright scams. One of the things you mentioned before we went on is be cautious if someone’s asking you to put money upfront, or if it’s a nonmedical facility. What are some things that people should watch out for?
Dr. Pollyea:
Yeah. So, one of the things that is so important in our area is clinical trials and participating in clinical trials. Patients who opt to do this and receive experimental therapies can sometimes get the treatment of the future, get a drug that’s not currently available through the FDA, but may have a lot of promise.
And this is the way that we fight this disease. We’ve recently had an onslaught of approvals for AML and that’s because the patients being willing to participate in sanctioned clinical trials. So, participating in a sanctioned clinical trial is crucial, and it’s always a recommendation of all leukemia doctors.
When you participate in a conventional clinical trial, you’re asked to sign a consent form that explains what you’re doing and why. There is a confirmation that this has been vetted by an institution’s regulatory board that is prioritizing the safety and well-being of you, the patient. This has been approved by the FDA as a clinical trial. Nobody would ever ask you to pay money. That’s not ethical to participate in a clinical trial. Insurance covers whatever standard of care. And the clinical trial covers anything that isn’t.
So, if you find yourself in a situation where you’re not being asked to sign a consent form, where a clinical trial has not been reviewed by a regulatory board, where your doctor is not a leukemia specialist, where the FDA has not sanctioned the treatment, all of those are alarm signs.
Because there are people out there that are preying on patients in a desperate situation, a very difficult time in their life, and giving them sort of false hope and leading them down paths that are not legitimate.
One easy thing to do to sorta check to see if a clinical trial is legitimate is to go onto clinicaltrials.gov.
This is a resource set up by our national healthcare system that now feeds in every legitimate clinical trial from all over the world, needs to be registered on clinicaltrials.gov. So, if you can’t find your clinical trial on clinicaltrials.gov, I would have a lot skepticism and caution about that.
Ross:
Like what advice do you have for people when they’re first diagnosed? What are the first things they should try to do?
Dr. Pollyea:
Yeah. I mean, that reaction is totally normal and natural. I mean, many times these people are perfectly healthy or have been perfectly healthy, and this news is a complete shock.
And so, it is normal and appropriate to have some period of grieving for the healthy life that you are losing. But I would also, while giving yourself that time to grieve, first, draw on your support system, your family, your friends. Allow them to help you. Accept that assistance that they have. And to be optimistic because we are getting so much better at treating this disease.
I had mentioned before, there has been an onslaught of approvals for drugs in this area the likes of which hasn’t been seen in decades. We have new tools and weapons in our arsenal that we couldn’t have dreamed of even a few years ago.
We in our community are very excited and hopeful about the future and we hope that that will translate ultimately to patients, but being depressed or being down, being scared, all of that is normal.
All of that is expected. Anyone would feel like that. Allowing yourself to have those feelings and emotions is important, as long as it doesn’t get in the way of doing what you need to do to fight this disease.
Ross:
It sounds like you’re hopeful about new treatments for the disease. How about a cure? What’s the science? What’s the medical science say about that? Are we getting any closer to that?
Dr. Pollyea:
We are getting closer to curing this in more cases. So, like I mentioned before, as bad as this is, we can already cure some subsets of patients. There’s one type of Acute Myeloid Leukemia called Acute Promyelocytic Leukemia, APL. It’s an uncommon form of AML, less than 10 percent.
But we can cure close to 99 percent of people with APL. And APL, 15 years ago, was universally the worst form of acute leukemia to get. So, that dramatic 180 that we’ve seen in APL, we are hoping to translate into other forms of AML.
Some other forms of AML have cure rates as high as 50 percent, 60 percent, 70 percent in the right setting. Sometimes we can cure patients with a stem cell transplant fairly reliably. So, we are very, very hopeful about our ability to continue to make progress and cure more and more and more of these patients. That’s the future that we see.
Ross:
Dr. Pollyea, thank you so much. And thank you so much for ending on such a positive note. We really appreciate it. And thank you for joining us for this program today.
To learn more about AML and to access tools to help you become a proactive patient, visit powerfulpatients.org. I’m Ross Reynolds. Thanks for joining us.
https://powerfulpatients.org/wp-content/uploads/Pollyea-1.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-06-05 15:38:122022-09-08 12:04:58Fact or Fiction? AML Causes & Symptoms
Last week, we hosted an Empowered #patientchat on finding your voice and what stops patients from seeking a second opinion.
A second opinion is crucial to prevent misdiagnosis or unnecessary procedures or surgeries. A study done by Mayo Clinic showed that as many as 88% of patients who get a second opinion go home with a new or refined diagnosis. That shows that only 12% of patients receive confirmation that their original diagnosis was complete and correct. Still, a lot of patients never get second opinions. So, we wanted to chat about this and see what the Empowered #patientchat community had to say, and these were the main takeaways:
The Top Tweets…
Full Chat
https://powerfulpatients.org/wp-content/uploads/Finding-You-Voice-patientchat-Highlights.png600600Kara Rayburnhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngKara Rayburn2019-02-01 16:44:322024-01-24 14:09:32Finding Your Voice #patientchat Highlights
The term “patient empowerment” is among the top buzzwords in health care circles, but as with many buzzwords, they can mean different things to different people. The term is most often used to emphasize the value of having patients assert greater control over their health and health care. WHO defines empowerment as “a process through which people gain greater control over decisions and actions affecting their health” (WHO 1998). This shift is due in large part to the use of technology that facilitates increased patient access to information via the Internet, peer-to-peer sharing, consumer health devices, and mobile apps.
In a recent Twitter chat, I set out to explore what it means to be an empowered patient today. The global participation of those who shared their views on the topic shows that patient empowerment is something of universal interest.
Seven Essential Components of Patient Empowerment
1. Information
Information is fundamental to the process of patient empowerment. Rare disease advocate and parent, Anne Lawlor (@22Q11_Ireland) believes that “an informed educated parent is an empowered one.” Patients make the best decisions when armed with the right information. To make genuinely informed decisions about our treatment we must have access to the relevant information needed to make those decisions. “Being informed is key to empowerment for me,” says specialist palliative care social worker, Deirdre McKenna (@KennaDeirdre). “Accurate information, clearly communicated and an available space to discuss and explore options and choices.”
Research shows that access to the right information, at the right time, delivered in the right way, leads to an increase in a patient’s desire and ability to take a more active role in decision-making. Open and transparent communication and access to a patient’s own medical records is a key driver of patient empowerment. Medical Director and Consultant Surgeon, Dermot O’Riordan (@dermotor) believes to truly empower patients “we should be aiming for the “Open Notes” principles of default sharing of all documents.” As patient advocate and CEO of Medistori Personal Health Record, Olive O’Connor (@MediStori) points out, “the patient is at the very core of every single service they use – they know everything there is to know about themselves, in the home and outside of it. Yet patient records are not kept with them!”
The OpenNotes initiative began in 2010 as a year-long demonstration project, with 105 primary care physicians at three diverse U.S. health care centers inviting 20,000 patients to read visit notes online through patient portals. Findings from the study suggest that shared notes may improve communication, safety, and patient-doctor relationships, and may help patients become more actively involved with their health and health care. Evidence also shows a sixty percent improvement in the patient’s ability to adhere to medications, a major problem with managing chronic pain conditions. What is key to the discussion on patient empowerment is that this initiative “demonstrates how a simple intervention can have an enormous impact, even absent advanced technology” (my emphasis).
2. Health Literacy
While access to information is a key driver of patient information, health literacy is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions.” (National Library of Medicine). Health literacy should come before digital literacy. “Health literacy is crucial,” says healthcare analyst, Matthew Loxton (@mloxton), “and you cannot get empowerment without health literacy.” Soo Hun (@soo_cchsc), Programme Manager at the Centre for Connected Health and Social Care, believes “digital is a key aspect but health literacy, even basic literacy is a must. Not all things digital requires tech know-how but all health information requires basic literacy. An app for meds reminder is no use if a patient lacks understanding of why medication is needed in the first place or why they need to be taken promptly. We spend too little time transferring knowledge to patients.”
This transfer of knowledge is crucial to the empowerment process, according to Olive O’Connor. “At the first point of contact with the patient,” she says, “education on how, what, why, where and when in relation to a condition or medication should be talked through fully. All other tools (digital, leaflets etc.) should come after the conversation which is key to empowerment.”
3. Digital Literacy
Cornell University defines digital literacy as “the ability to find, evaluate, utilize, share, and create content using information technologies and the Internet.” It’s interesting to note that opinions vary on whether digital literacy is essential to patient empowerment. RN turned patient advocate and health activist, Kayoko Ky Corbet (@kkcorbet) doesn’t believe that “digital literacy is an absolute requirement, but the ability to find accurate relevant information, and understand the information is.” Breast cancer advocate, Jennifer (@vitalfrequencis) agrees that “digital literacy is not fundamental and should not be part of the equation. Empowerment needs to be across all socioeconomic groups. Otherwise…a whole bunch of patients may never be empowered.”
Dermot O’Riordan is convinced that “whilst it sounds nice to say that digital is not ‘necessary’ for patient empowerment, in practice it is going to be pretty tough to do it properly/completely without digital.” Transplant recipient and rare disease patient, Carol McCullough (@Imonlyslightly ) also believes “digital literacy strengthens the empowerment process.” She too points to “access to your medical information online” as a key component of the empowerment process. “Knowing your personal medical data is strength, as is education about your illness,” she says.
Maternity campaigner, SeánaTalbot (@SeanaTalbot) believes that “those with long-term conditions and access to technology have a better chance of accessing information and support.” Indeed many patients have found in the online world of peer-to-peer healthcare an environment in which they are supported to become a more empowered participant in their healthcare. As I look back on my own empowerment journey, my progress was advanced step-by-step by learning more about my disease initially from doctors, then through Internet searches, and most helpful of all through patient peers online. Finding and being part of a patient community can be an important step on the path to empowerment.
4. Self-Efficacy
Self-efficacy, as it relates to healthcare, is belief in your ability to effect change in outcomes so that you can achieve your personal health goals. The patient empowerment definition which comes to us from the European Patient Forum describes empowerment as a process that “helps people gain control over their own lives and increases their capacity to act on issues that they themselves define as important.”
Developing a sense of personal control over your health is in itself empowering. The empowered patient is confident in their ability to manage their condition. When unsure about where to go or what to do next they will feel confident to ask questions of the healthcare professionals providing their care. This confidence comes easier to some than others, and even the most confident may need guidance from their doctors in managing their disease. Endocrinologist, Iris Thiele Isip Tan, MD (@endocrine_witch) points out that “some of my patients are surprised when I teach them how to adjust/titrate insulin doses. Apparently not all MDs ‘allow’ this. Some need handholding because they get anxious about the responsibility.”
Digital leader and physiotherapist, Linda Vernon (@VernonLinda), believes “for authentic patient engagement to occur, we need to establish what the patient brings to the table, something akin to an individual, personal take on Asset-Based Community Development – perhaps we could think of it as Asset-Based Personal Development, supporting the patient to tap into their own internal, community or environmental resources to improve their health and wellbeing. Engaging patients should be as much about exploring what they can do for themselves and to help the health and care system, as what we professionals can offer to the patient.”
5. Mutual Respect
The healthcare professional is the most important contact point for the patient and the system and (dis)empowerment often manifests in the patient/professional relationship. At the heart of the empowerment approach is seeing the patient-professional relationship as a partnership of equals. Carol McCullough describes it as a reciprocal process of “mutual respect for what each person knows and being allowed to make informed choices. It is not about command and control.”
This is a partnership approach that seeks to balance clinician expertise with patient preference. It recognizes that while healthcare professionals are the experts in their knowledge of a disease, patients are the experts by experience. The empowerment process is about sharing both knowledge and experience to set new goals and learn with and from each other. Dr Kit Byatt (@Laconic_doc) agrees. “Many patients are experts”, he says, “especially rare disease patients. I’ve learned from many in my career.”
Building better relationships and seeing the patient as more than ‘just a patient’ was a recurring theme in the Twitter chat. Elena Vaughan (@StigmaStudyIE), who is researching the impact of HIV-related stigma in Ireland, believes that “an empowered patient is treated with respect, involved in shared decision-making regrading care and treatment, and is not patronised. For people with chronic conditions, effective communication, continuity of care and establishing a relationship of trust is very important.” Sometimes, as ME blogger and patient advocate, Sally Burch (@KeelaToo) points out, “not all patients are lacking confidence to speak. The problem is being heard.”
Patient and community advocate, Triona Murphy (@Murpht01) advises doctors to get to know your patients as individuals. “Know your patient!!…and their family,” she says. “No one size fits all! BUT there was/is still a culture of the ‘person’ stops at the door of the hospital and that person is now a patient.’” As antibiotic resistance campaigner, Vanessa Carter (@_FaceSA) says, “I might be a patient but I am also a creative director by profession. No one recognises me on that level. They see me as an underdog.”
6. Shared Decision Making
This partnership approach allows for Shared Decision-Making (SDM) – the conversation that happens between a patient and clinician to reach a healthcare choice together. Examples include decisions about surgery, medications, self-management, and screening and diagnostic tests. There is ample research which suggests that health outcomes are better in patients who are more involved in decisions about their treatment.
In the SDM model, the clinician provides current, evidence-based information about treatment options, describing their risks and benefits, and the patient expresses his or her preferences and values. Matthew Loxton points to how seldom we have metrics to track whether patient goals are being met. “Yet this,” he believes, “is THE most important part of quality.”
7. A Facilitating Environment
Linda Vernon defines patient engagement as “activating the person’s inner assets and supporting them to make the best use of them.” Being supported is a key component of patient empowerment. Many patients would like to take more responsibility for their own health and care, given the opportunities and support to do so. Empowerment does not happen in a vacuum: it is a two-way process. The patient needs a counterpart in the health professional who welcomes the patient’s involvement and knows how to create an enabling healthcare environment. Kayoko Ky Corbet states she became an independent patient advocate when she realized most doctors simply do not have the time (and often skills) to take this facilitating role and promote shared decision-making that patients desperately need. As Patient Critical Co-op (@PatientCritical) puts it, “if you have a patient who wants to advocate for themselves, and become informed, you also need a doctor that respects the patient’s right to share decision making.”
Is It Empowerment or Participation?
Not everyone likes to use the term “empowerment”, as it implies that it is an authority given to someone to do something. “I balk at the idea that professionals can ‘give’ (usually on their terms) power to the powerless,” says Alison Cameron (@allyc375). “We need to create conditions whereby people can “empower” themselves.” Seána Talbot agrees that patient empowerment “doesn’t mean ‘giving’ people power.’ Rather it’s about ‘enabling’ them to recognise and use their power.”
Perhaps the term ‘participation’ (which is a more active state) is preferable? This distinction is important because empowerment cannot be imposed ‘top down’ (although it can be facilitated). Sharon Thompson (@sharontwriter) believes that “patients should not be pressurised or need to be in a position of ‘power.’ It should be automatic that a patient is central and key to their care. Patients are automatically empowered when they are respected as being people who are entitled to understand and know about their care.”
Neither is patient empowerment about the patient taking full control or shifting responsibility to the patient. “If the empowerment amounts to abandonment”, says Matthew Loxton, “then the patient’s health goals are not being met. Patient empowerment should never be an excuse for abandoning or burdening the patient.”
Rather, the empowerment approach, as defined by the European Patient Foundation (EPF) “aims to realise the vision of patients as ‘co-producers’ of health and as integral actors in the health system.” Caregiver Reinhart Gauss (@ReinhartG) agrees that “patient advocates want to work with not against doctors – to share experiences and to grow in knowledge.” Vanessa Carter is clear that “we still want our doctors, but they are not there 24/7 so patients need the right tools to make self-care possible.”
Equally, it is about recognizing that there are degrees of involvement and not all patients wish to be ‘empowered.’ There is a spectrum of interest in wanting to assume an active role in care – from being passively receptive to fully engaged. It is up to the patients themselves to choose their own level of engagement. Pharmacist Chris Maguire (@chris_magz) sees this choice as the essence of empowerment. Patients “get to decide how much they want to look into things and take control. Or they want to be guided on the journey and have trust in their healthcare providers. But the key is that they decide the level of interaction and are not dictated to.” Kayoko Ky Corbet agrees that “true patient empowerment should be about helping patients get involved at their highest potential or at the level they choose.” However, she says “it’s also important to keep the option of involvement open. Ideally patients should get opportunities to change their minds to participate in decision-making later.”
Empowerment as an Ongoing Process
Empowerment is a non-binary, non-linear process. Your needs may change over time. You might feel empowered in a certain context, but disempowered in another. Healthcare communicator, Michi Endemann (@MichiEndemann) makes the distinction that “talking about empowerment as a healthy person is quite different than talking about it as a patient.” As patient advocate, Rachel Lynch (@rachelmlynch) puts it, “it can be quite tiring being empowered when all you want to be is well.” A sentiment echoed by Kathy Kastner (@KathyKastner), founder of Best Endings, who clarifies how “to me ‘empowered’ assumes I’m feeling physically and mentally up to the task of ‘being engaged’. I’ve seen powerhouses who cannot bring themselves to take responsibility for their own health.”
Mental health advocate and co-founder of #DepressionHurts, Norah (@TalentCoop) calls attention to the fragile nature of empowerment. “Even the strongest can quickly feel disempowered by a deterioration in health,” she says. “Fear disempowers. Sometimes it’s a case of ‘can’t’ not ‘won’t.’”
For those who feel ready for a greater degree of participation in their healthcare (and that of their family and loved ones), Jennifer advises that “being willing to self-advocate, along with self-confidence, communication skills, compromise, research skills, and relationship building” are some of the key traits and skills you need to become an empowered patient. Terri Coutee (@6state), patient advocate and founder of DiepCjourney Foundation, adds that “empowered patients do their research, ask questions, go to appointments organized, and take a friend to help listen.”
Barriers to Patient Empowerment and Overcoming Challenges
What are some of the current barriers to involving patients more in their care? Jennifer points to a “lack of adequate time during the doctor’s visit (on both sides), language barriers, technology barriers, generation gaps, and cultural gaps.” The solution? “All solved by building good relationships,” says Jennifer.
Norah also calls attention to the technology barriers. “For older patients simple things like communication (hearing), or uninformed changes are extremely disempowering; as is over reliance on technology for a generation who may not have ‘tech’ understanding or access.” Tim Delaney (@FrancosBruvva), Head of Pharmacy at a leading hospital in Ireland highlights the fact that “in acute hospitals we treat huge numbers of elderly people whose engagement with social media and new technology is lower. We need to design technology that meets their usability needs AND use whatever suits them best be it old tech or new.” Soo Hun agrees that “the tech savvy few have quicker and better access to health information and therefore can have choice and autonomy. To reverse that we need to make technology ubiquitous and make health information and choice easily accessible.”
Whilst Vanessa believes it should be “governmental policy to have digital resources in place, for example, disease specific websites / apps supported by health authorities,” Kayoko believes it can start with “tech-savvy advocates (like me) who could help patients learn to use simple digital tools.”
Matthew Loxton sees a core barrier to empowerment to be “the large knowledge/power gradients between patients and health care providers. Without access to their data, trustworthy sources of medical knowledge, and the power to execute their choices in achieving health goals, empowerment is an empty phrase.” Triona Murphy echoes this systemic challenge by clarifying that “the whole system needs to understand the patient’s right to be equal partners in their care. IF that is what the patient wants.”
Sometimes the fear of being labelled a difficult patient can be a barrier to empowerment. “Some patients feel uncomfortable challenging the judgement or actions of their caregivers for the fear of being labelled as ‘difficult’, of offending staff and/or because of concerns of compromising their healthcare and safety,” says Tim Delaney.
Final Thoughts
Not everyone wants to be empowered in making decisions about their care, and not every doctor wants to take the time. Some doctors use medical terminology which is incomprehensible to patients, while some patients have low health literacy skills or come from cultural backgrounds that lack a tradition of individuals making autonomous decisions. That said, Carol McCullough points out that while “not everyone may want to be empowered, for the health service to be sustainable, more people are going to have to take on more responsibility.”
Medical Doctor and Chair of Technical Advisory Board, Pavilion Health, Dr Mary Ethna Black (@DrMaryBlack) points to the inevitability of the shift towards patient empowerment. “Empowerment is an inevitable shift that is happening anyway, “she says. “We cannot turn back the tide or turn off the internet.”
Kayoko Ky Corbet agrees that we “must understand that patients making informed decisions is the ultimate way to reduce waste, pain and regrets in healthcare. It’s also morally the right thing to do!” Patient Critical Co-op also believes in the moral imperative that “empowerment essentially means a group or society recognizing your right. Patient empowerment exists as an action patients can take to improve themselves, but the key to achieving that improvement is having a group, organization, or state enshrine and recognize those rights.” In fact, the Alma Ata Declaration defined civic involvement in healthcare as both a right and a duty: “The people have the right and duty to participate individually and collectively in the planning and implementation of their healthcare.” The Declaration highlights the collective dimension of empowerment and the importance of action towards change. By working together to think internationally and act nationally we can draw on each other’s experiences so that as individuals and as a collective we can work towards better outcomes for all patients. To quote Terri Coutee, “When we gather our collective empowered voices, we feel a strong responsibility to give voice to others.”
I would like to acknowledge the assistance of Dr Liam Farrell in facilitating the Twitter discussion on which this article is based.
A Stanford Medicine X e-Patient scholar, Marie Ennis O’Connor is an internationally recognized keynote speaker, writer, and consultant on global trends in patient engagement, digital health and participatory medicine. Marie’s work is informed by her passion for embedding the patient voice at the heart of healthcare values. She writes about the experience of transitioning from breast cancer patient to advocate on her award-winning blog Journeying Beyond Breast Cancer.
https://powerfulpatients.org/wp-content/uploads/What-Does-It-Mean-To-Be-An-Empowered-Patient_.png600600Marie Ennis-O'Connorhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngMarie Ennis-O'Connor2018-05-22 17:22:012024-01-24 14:22:02What Does It Mean To Be An Empowered Patient?
The news that you, or a loved one, has a serious illness can be a terrible blow. You may be faced with an array of emotions ranging from shock to fear to anxiety. You will likely have many questions and concerns about what the coming days and months will bring, and the impact living with this illness will have on your life and the lives of your family. Although you may be reeling from the news, it’s important that you learn as much as you can about your diagnosis, its symptoms, how it may progress and what treatment options are available. In this article, you will learn which questions you should ask your healthcare team and where to find reliable and trustworthy information to become better informed about your health condition.
1. Obtaining Information From Your Doctors And Healthcare Team
Having answers to your questions can help you understand your illness better and feel more in control about your treatment decisions. How much information you want is up to you. Some patients feel overwhelmed by too much information at this stage. Others say they didn’t receive enough information. While information upon first diagnosis is vitally important, you may be in shock and in a heightened emotional state which makes it difficult to fully comprehend all the information you are given. If possible, bring a trusted friend or family member to appointments with you to take notes. If this is not possible, ask your doctor if you can record the consultation so you can focus on listening, and go back and review what was said later.
Medical care is a conversation and to have influence in that conversation you have to speak up. Never be embarrassed to tell your healthcare team if you don’t understand something they’ve said. Sometimes doctors use medical jargon without realizing they are not explaining things in terms we understand. Repeat what the doctor has told you to be sure you understand and ask for clarification if needed.
Some questions to ask your doctor about your diagnosis:
What are the symptoms of this illness?
What should you do if you notice new symptoms or if existing symptoms worsen?
Do you need any further diagnostic tests?
What are your treatment options?
What are the side-effects of the recommended treatment?
What are the benefits vs the risks?
What happens if you do nothing?
Are there other treatment options available?
Finally, ask your healthcare team if they can recommend further reading, support groups and other resources to help you learn more about your illness.
2. Finding Reliable Information Online
As you move along the patient journey and better understand your illness, you may want higher levels of information. However, you may find the information healthcare professionals provide has not keep pace with your increased needs. This is the point where many patients turn online to seek more information. While the Internet can be a useful source of health information, it’s important to know how to critically evaluate the information you find online. Always discuss what you find with your healthcare team and ask them to put the information into context for your particular situation.
Here are some questions to help you determine the trustworthiness of online sources of information.
Who has produced the information?
Does the organization have commercial interests or another reason they are promoting this information?
Is the name of the organization and their aims in setting up the website clearly shown?
Does the site provide contact details if you have any questions?
Is the information on the website up to date?
Does it cite the source of the information that is being presented?
Does the site link with other reputable sites that give similar information?
3. Evaluating Medical News Reports
Whether it’s published in hard copy or online, medical news reports can mislead people into thinking a certain drug or treatment is the next breakthrough in a disease. As patient advocates we must learn to read beyond the headlines to filter out the good, the bad, and the questionable.
The following questions will help you evaluate the reliability of medical news reporting.
Does the article support its claims with scientific research?
What is the original source of the article?
Who paid for and conducted the study?
How many people did the research study include?
Did the study include a control group?
What are the study’s limitations?
If it’s a clinical trial that is being reported on, what stage is the trial at?
Always try to read an original study (if cited) to critically evaluate the information presented. Understanding research literature is an important skill for patient advocates. For tips on how to read a research paper click on this link.
4. Learning From Peers
From helping us to uncover a diagnosis and finding the right doctors and treatments, to learning about everyday coping tips, turning to our peers can make all the difference in how we live with our illnesses. Much of this peer-to-peer learning takes place through social media discussions on patient blogs and in Facebook groups and Twitter chats. On Facebook you can connect with other patient advocates and join Facebook groups related to your disease or health condition. On Twitter you have a greater mix of patients, physicians, healthcare professionals and medical researchers coming together to discuss healthcare matters. It is becoming increasingly popular for attendees at key medical conferences, such as ASCO, to “live-tweet” sessions. You can follow along on Twitter using the conference hashtag which you should find published on the conference website. Another way to learn on Twitter is to join a Twitter chat related to your health condition. Twitter chats can be one-off events, but more usually are recurring weekly chats to regularly connect people. There are chats for most disease topics and a full list can be found by searching the database of the Healthcare Hashtag Project.
Being an advocate involves asking lots of questions, conducting your own research, and making your preferences known to your healthcare team. By doing this, you will be better informed and in a stronger position to get the treatment that is right for you. If this feels overwhelming to you right now, go at your own pace, and reach out to others who have walked this path before you. There is an army of patients who are standing by, ready to share their healthcare wisdom and practical coping tips with you. Seeking their advice will help lessen the fear and isolation you may be feeling, give you a sense of shared experience and connection, and help you feel more in charge of your healthcare decisions.
A Stanford Medicine X e-Patient scholar, Marie Ennis O’Connor is an internationally recognized keynote speaker, writer, and consultant on global trends in patient engagement, digital health and participatory medicine. Marie’s work is informed by her passion for embedding the patient voice at the heart of healthcare values. She writes about the experience of transitioning from breast cancer patient to advocate on her award-winning blog Journeying Beyond Breast Cancer.
Do clinicians have accurate expectations of the benefits and harms of treatments and screening tests?
A new study in JAMA Internal Medicine concludes not. In a systematic review of 48 studies (13 011 clinicians), the researchers found that clinicians rarely had accurate expectations of benefits or harms, more often underestimating harms and overestimated benefits. Among the findings, obstetricians and neurologists underestimated the risk of birth defects from anti-epileptic drugs and GPs overestimated the benefit of prostate cancer screening. Transplant surgeons were biased towards an inaccurately low estimate of graft failure and all types of doctors were unaware of the risk of radiation exposure from imaging.
What do these findings mean for patients? Inaccurate clinician expectations of the benefits and harms of interventions can profoundly influence decision making and the standard of care patients receive. Patient activist, blogger, and author of the upcoming book “Heart Sisters: A Survivor’s Take on Women and Heart Disease” (Johns Hopkins University Press, November 2017), Carolyn Thomas, believes this to be “a consistently systemic issue for patients, too: most believe medical interventions will help more/harm less than they actually do”. It’s a wake-up call for patients who have a critical role to play in understanding and weighing up benefits and risks for ourselves, in order to get better treatment. And it’s a further reminder of the importance of shared decision making to reach a healthcare choice together, as opposed to clinicians making decisions on behalf of patients.
However, understanding the risks associated with a treatment is not necessarily straight-forward. The challenge for busy clinicians is that there isn’t always the time to read and digest the latest research to inform their practice. Medical commentator, physician, and cancer survivor, Elaine Schattner, believes that because medical knowledge changes so rapidly it’s hard for clinicians to keep pace. “This may be especially true in oncology,” she points out, “as patients become expert in their own conditions and needs, they may prefer to look up information on their own, and share their findings with their physicians.”
A lengthy article published this month in ProPublica, examines what it calls “an epidemic of unnecessary and unhelpful treatment” requested by patients and delivered by doctors, even after current research contradicts its practice. “It is distressingly ordinary for patients to get treatments that research has shown are ineffective or even dangerous”, writes David Epstein. “Some procedures are implemented based on studies that did not prove whether they really worked in the first place. Others were initially supported by evidence but then were contradicted by better evidence, and yet these procedures have remained the standards of care for years, or decades.” Epstein points to a 2013 study which examined all 363 articles published in The New England Journal of Medicine over a decade — 2001 through 2010 — that tested a current clinical practice. Their results, published in the Mayo Clinic Proceedings, found 146 studies that proved or strongly suggested that a current standard practice either had no benefit at all or was inferior to the practice it replaced. Of course, this is not to say that myriad treatments don’t indeed improve and save lives, but it’s important to ask questions and do your own research before making a decision on which treatment is the best for you.
Start by asking your doctor to explain all the treatment options open to you, including what would happen if you do nothing. Recognise that all treatments are inevitably associated with some risk of possible harm. Ask your doctor to quantify that risk beyond a purely descriptive term, such as “low risk” (what your doctor considers a small and acceptable risk may be unacceptable to you). Next, do your own research. In order to make an informed decision, you will need to gather reliable information on which to base your choice. Fully exploring the risks and benefits of treatment involves doing your own evidence-based research (using evidence from medical studies that have looked at what happens to many thousands of people with your condition). In a previous article, I shared with you some helpful guidelines for assessing medical information. Most media reports about the benefits of treatments present risk results as relative risk reductions rather than absolute risk reductions, so you will need to understand the difference. Absolute risk of a disease is your risk of developing the disease over a time period. We all have absolute risks of developing various diseases such as heart disease, cancer, stroke, etc. Relative risk is used to compare the risk in two different groups of people. For example, research has shown that smokers have a higher risk of developing heart disease compared to non-smokers. Ask your doctor to differentiate between absolute and relative risk. Check out the NNT website which provides non-biased summaries of evidence-based medicine. “NNT” stands for a statistical concept called the “Number-Needed-to-Treat” – as in “How many patients need to be treated with a drug or procedure for one patient to get the hoped-for benefit?” The core value of the NNT is its straightforward communication of the science that can help us understand the likelihood that a patient will be helped, harmed, or unaffected by a treatment. It provides a measurement of the impact of a medicine or therapy by estimating the number of patients that need to be treated in order to have an impact on one person. Because we know that not everyone is helped by a medicine or intervention — some benefit, some are harmed, and some are unaffected, the NNT tells us how many of each.
You may also want to hear about what other people with your condition have chosen to do and what their experience has been. But remember that just because something has/hasn’t worked for someone else, it doesn’t mean it will/won’t work for you. Orthopedic surgeon, Dr Nicholas DiNubile, recommends patients ask their doctors, “If this were you, or one of your immediate family members, what would you do and/or recommend?” While this may be useful, you must ultimately decide what benefits and risks are important to you. Can you tolerate the side-effects? Are you happy with the way the treatment is administered? Would you find it stressful to live with the risk of any serious side effects, even if the risk is small? What matters is whether you think that the benefits outweigh the risk of any side effects. Everyone is different. The treatment recommended for you may not be the best treatment for your particular lifestyle. Being an advocate for your own health care involves asking lots of questions, doing your own research, and making your preferences known to your doctor. By doing this, you will be better informed and in a stronger position to get the treatment that is right for you.
A Stanford Medicine X e-Patient scholar, Marie Ennis O’Connor is an internationally recognized keynote speaker, writer, and consultant on global trends in patient engagement, digital health and participatory medicine. Marie’s work is informed by her passion for embedding the patient voice at the heart of healthcare values. She writes about the experience of transitioning from breast cancer patient to advocate on her award-winning blog Journeying Beyond Breast Cancer.
https://powerfulpatients.org/wp-content/uploads/2017/02/Screen-Shot-2017-02-24-at-12.46.03-PM.png406722Marie Ennis-O'Connorhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngMarie Ennis-O'Connor2017-02-24 17:55:492024-06-24 14:13:34How to Weigh Up the Benefits and Risks of Treatment…and Why It’s Important That You Do
The ePatient virtual classrooms are designed to empower patients in all their healthcare matters.
ePatient 101
ePatient101: How to be an Empowered Patient, is an online course for anyone interested in becoming an empowered patient, empowered caregiver, or patient advocate. Through this online course taught by Alex Barfuss, you will learn:
The meaning of the term “ePatient”
Why being an ePatient is so important in today’s healthcare system
How you can save time and money and get better overall value from your health care providers
How to advocate for yourself
Tools, tips and best practices to help manage your or your loved one’s chronic disease
Caregiver 101
Caregiver 101 is full of useful tools for caregivers and taught by Caregiving.com founder, Denise Brown. By taking this course, you will learn:
How the carer/caree relationship can be a health relationship
How to find balance
How to find more time for your self
How to ask for support
Tips, tools, and tactics to be a better carer/caree
Curated links and resources
Videos
Knowledge quizzes
Support from a community of caregivers at cargiving.com
Chronic Lymphocytic Leukemia (CLL) 101
We are excited to be partnering up with Intake.me to bring you CLL 101. We wanted anyone struggling with a recent CLL diagnosis to become empowered through knowledge and support. By taking this course, you will receive:
An overview of CLL
Facts about CLL
Curated links and resources
Videos
Knowledge quizzes
Printable checklists with questions to ask your doctor
Why you should immediately get a second, expert opinion
Tips on building your healthcare team, and how your local doctor can work with a CLL expert to provide the best treatment
Where to find the latest CLL research, clinical trials, and other treatment options
Ability to ask questions from other CLL 101 students
These courses are part of the Intake.me experience and are free to everyone. You can sign up be clicking one of the buttons below. Enjoy!
Have you ever had the experience of leaving the doctor’s office wishing you had remembered to ask a certain question? Or have you left it until the very end to tell your doctor about the real reason for your visit? These so-called “doorknob” questions – bringing up an important concern just as you are leaving the office – can mean your doctor won’t have time to adequately address your concerns. When the average time it takes for a doctor’s visit is fifteen minutes, it’s easy to feel rushed and forget what you wanted to say, or to leave an appointment unsure of the information you have heard. But with a little advance preparation you can learn how to make the most of those fifteen minutes. Follow these fifteen tips to become a more empowered and engaged partner in your own health – and the health of those you care for.
1. When you call to make your appointment, explain clearly why you need to see the doctor. Let the receptionist know how much time you will need to schedule for the visit. If you have any special needs, such as wheelchair access or interpretive needs, let the office know in advance.
2. Be sure to that where you make your appointment accepts your insurance. You can call or go online to your insurance website to see a directory of in-network providers.
3. If this is your first visit to a new physician, gather together any past medical records and family medical history to take along with you. If you’re seeing other doctors and have information they’ve provided, bring this along too.
4. Write down a list of your symptoms before the visit. It’s a good idea to keep a diary so you can chart your symptoms over time. Include details of the type of symptoms you are experiencing, when these symptoms began, and what makes them better or worse.
Scale (“How bad is it? How much does it affect you?”)
Timing (“When did it start? How long does it last? Does it come and go? Is it gradual or sudden in onset? What makes it better or worse?”)
Other (“Any other symptoms?”)
5. Set the agenda at the start of your visit. Did you know that a patient has an average of 23 seconds to state their concerns before a physician interrupts? According to an article published in The Journal of the American Medical Association, only 28% of doctors know their patient’s full spectrum of concerns before they begin to focus on one particular concern, and once the conversation is focused, the likelihood of returning to other concerns is only 8%. Doctors have a limited amount of time for office visits. In order to use their time wisely they usually set the agenda and control the visit as much as possible. To avoid this happening to you, prepare in advance the top two or three concerns you want to raise with your doctor. Are you looking for a diagnosis? Do you need a new treatment plan or a modification of an existing plan? Are you looking for help with feelings of fatigue or depression? Don’t forget to describe your emotional state and any personal circumstances which may influence your physical health. Write down your main concerns so you are ready to verbalize them clearly at the beginning of your visit.
6. If you use a self-tracking device, like a Fitbit, download your data and summarize the findings beforehand.
7. Bring a list of all medications you are currently taking, including over-the-counter medications, vitamins, herbs, or supplements. If you have a smart phone or tablet, it’s useful to take pictures of your medication and supplement labels to show the doctor.
8. During your visit, tell your doctor you would like to take notes. If you would prefer to record your notes via your smartphone, ask your doctor if it is ok to do so.
9. Medical care is a conversation. So to have influence in that conversation you have to speak up. If you don’t want the treatment your doctor recommends (or you’re not sure), it’s reasonable to ask if there are other treatment options available. Never be embarrassed to tell your doctor if you don’t understand something she has said. Sometimes doctors use medical jargon without realizing they are not explaining things in terms we understand. Repeat what the doctor has told you to be sure you understand and ask for clarification if needed
10. If you find it difficult to speak up for yourself, or you are facing a potentially challenging diagnosis, bring a friend or family member along for support. This person can also take notes and help you remember what was discussed later.
11. Always be honest with your doctor. You may not like to admit how much you drink, or smoke, or if you have stopped taking your medication because of expense or side effects, but your doctor needs to know about these and other lifestyle matters to ensure you are receiving optimum care.
12. Ask you doctor to explain any test results to you, Request a copy of the results for your own files.
13. Before you leave, be sure you understand what needs to happen next. Do you need any further diagnostic tests? When will you get the results? If you have just received a diagnosis, what are your treatment options? If you have questions or concerns later how should you contact your doctor? You can also ask if your doctor recommends any specific reading materials or websites about your condition.
14. If you have been given a prescription for a new medication, do you understand how and when the medication should be taken? Are there any side-effects, for example drowsiness, you should watch for? How will you know if the medication is working? What happens if you miss a dose?
15. After your visit, review and file your notes along with any test results or other documentation and billing you received. Schedule any follow up tests or appointments right away.
Your relationship with your doctor is one of the most important you have. Advance preparation will help you use your own time and your doctor’s time more efficiently and effectively. When people take an active role in their care, research shows they are more satisfied and do better in how well treatments work. Preparing for your doctor’s visit is an important step toward becoming a partner in your own health care and a better advocate for your health and well-being.
A Stanford Medicine X e-Patient scholar, Marie Ennis O’Connor is an internationally recognized keynote speaker, writer, and consultant on global trends in patient engagement, digital health and participatory medicine. Marie’s work is informed by her passion for embedding the patient voice at the heart of healthcare values. She writes about the experience of transitioning from breast cancer patient to advocate on her award-winning blog Journeying Beyond Breast Cancer.
https://powerfulpatients.org/wp-content/uploads/2016/12/Beauty.png800800Marie Ennis-O'Connorhttps://powerfulpatients.org/wp-content/uploads/New-Logo-300x126.pngMarie Ennis-O'Connor2016-12-27 15:18:302024-01-24 13:55:1815 Tips To Get the Most From Your Doctor’s Visit
 Find Your Voice Resource Guide
Find Your Voice Resource Guide Office Visit Planner
Office Visit Planner Why Speaking Up Matter: Tips From an AML Advocate
Why Speaking Up Matter: Tips From an AML Advocate





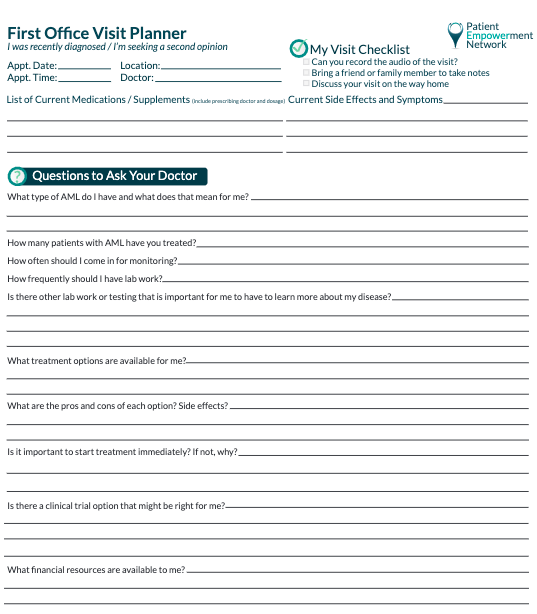
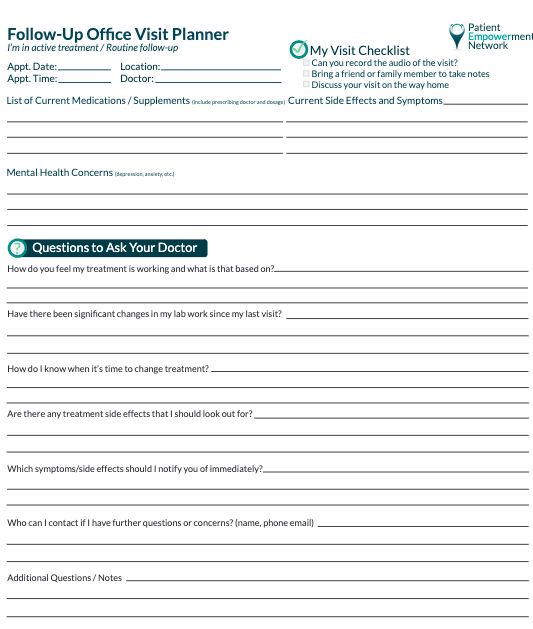




 Have you ever had the experience of leaving the doctor’s office wishing you had remembered to ask a certain question? Or have you left it until the very end to tell your doctor about the real reason for your visit? These so-called “doorknob” questions – bringing up an important concern just as you are leaving the office – can mean your doctor won’t have time to adequately address your concerns. When the average time it takes for a doctor’s visit is fifteen minutes, it’s easy to feel rushed and forget what you wanted to say, or to leave an appointment unsure of the information you have heard. But with a little advance preparation you can learn how to make the most of those fifteen minutes. Follow these fifteen tips to become a more empowered and engaged partner in your own health – and the health of those you care for.
Have you ever had the experience of leaving the doctor’s office wishing you had remembered to ask a certain question? Or have you left it until the very end to tell your doctor about the real reason for your visit? These so-called “doorknob” questions – bringing up an important concern just as you are leaving the office – can mean your doctor won’t have time to adequately address your concerns. When the average time it takes for a doctor’s visit is fifteen minutes, it’s easy to feel rushed and forget what you wanted to say, or to leave an appointment unsure of the information you have heard. But with a little advance preparation you can learn how to make the most of those fifteen minutes. Follow these fifteen tips to become a more empowered and engaged partner in your own health – and the health of those you care for.